 Review Article
Review ArticleAbstract
Changes taking place in healthcare require the involvement of everyone entities operating in the system. However, not all stakeholders have the same options for influencing system reform. It depends on many factors, such as ownership power, knowledge or the right tools. The most interested changes the group is patients, but their strength is relatively small. Quite differently the situation is, if we look at pharmaceutical concerns: definitely less interesting their changes and their potential for impact are much greater. The article presents what entities participate in introducing changes in health care and what are their real ones the possibilities of influencing the system and why these possibilities (or lack thereof) result.
Keywords: Stakeholders; Change; Health Care; Health Care System
Introduction
The necessity to introduce changes in health care, especially in the recent period, is not in doubt. However, this is not an easy or cheap task. For state and patient finances, for the health security of society, the situation of making changes requires constructive planning of the effects of change. Experts for several years show what changes would be beneficial, in which direction health care should be reformed, what solutions would bring the greatest benefits to all participants in the system. Observing changes in health care, it can be concluded that among many stakeholders operating in the system only some have a real impact on their introduction, type and course. The imbalance results from many factors related to the specificity of the system and its participants, the nature of changes and the political situation. The purpose of the work is to identify stakeholders who potentially have the greatest potential to influence the scope and course of changes in the healthcare system, and the sources of these possibilities.
Stakeholders
One of the difficulties of reforming the health sector is the large
number of entities that operate under the health care system. We
can call them health care stakeholders. Stakeholder theory was
initiated by the Stanford Research Institute in 1963, it concerned
organizations and proclaimed that stakeholders were groups
without whose support the organization could not function. Now in
1984, Freeman decided that stakeholders were all individuals and
groups in and around the organization that have an impact on the
organization’s goals or on which the organization could influence
achieving its goals [1]. Therefore, it should be recognized that
stakeholders will not be those units or groups that cannot influence
the organization. Stakeholders can also be divided into internal and
external. Internal is usually employees, management, shareholders
and the supervisory board. Customers are external, competitors,
suppliers, trade unions and state authorities [2].
It is believed [3] that the stakeholder theory can be applied
to public organizations. The main difference is that public
organizations operate in a highly politicized environment and the
choice of specific strategic reasons is dictated not by their actual
assessment, but by the bargaining power of the most influential
stakeholders. If we consider the fact that stakeholders in public
organizations have very unequal access to power, it may turn
out that selected groups not only influence the achievement of
the organization’s goals, but above all pursue their own goals.The introduction of fundamental changes in healthcare requires
identifying one of the leading stakeholders and thinking about how
they affect the introduction and course of changes in the system.
Stakeholders who may have an impact on health care include,
among others:
1. Politicians (minister of health, health committees,
parliament),
2. The payer (in Poland is the National Health Fund),
3. State healthcare institutions,
4. The management of health care institutions,
5. Private healthcare facilities,
6. Mid-level medical staff managed and
7. Patients.
These are not all entities, as there are many more in the health
care system and in its environment (e.g. insurers, pharmaceutical
companies, trade union and religious organizations, suppliers,
associations), however the authors mentioned can be considered
the most significant.
Changes in the Health Care System
In modern healthcare organizations, the changes have acquired a completely new character, ceased to be a specific event at a specific time, and have become a permanent process. The same situation occurs in Polish healthcare. For some time, all participants have been constantly experiencing new changes that involve very different aspects of the system’s functioning. This is not one big change in the whole system, but a string of introducing new solutions and innovations. This is not an easy situation for all interested parties. When making changes, the most important thing is to know what you want to change, plan the change, prepare people, make the change, and then control the adaptation. In practice, this is a very complicated process with many problems. Firstly, as a rule, there is no single idea for change, several variants of change methods are possible, and sometimes implementation in practice does not bring the planned effects. Secondly, changes always affect people, and this is the most unpredictable factor in the whole process. Changes disturb the existing order, raise fear of the unknown, threaten the economic situation and sense of security, and thus cause resistance from people to accept such solutions [4].
Most often the initiators of changes are individuals and small groups, and they concern large communities, sometimes entire societies. Health is the supreme value and is of great importance to people. The functioning of the system in which the state provides all health needs, because it has such an obligation, confirms the belief that health care is free, widely available. This results in such a high resistance of patients from introducing new solutions. They see any change as an attack on their rights to comprehensive “free” health services. However, it is difficult to expect a different perception of health protection in the event of an epidemic threat to the whole society. The changes also raise the concerns of medical and administrative staff, especially since unprotected solutions are replaced in a short time by other, quite different, which have to be learned during work, i.e. by experimenting on patients. Often, these are also changes that are subject to financial risk incurred by a doctor or pharmacist, and in this situation this burden is shifted to the patient who, in fact, has no choice. Certainly, participants’ resistance could be reduced by improving communication between decision-makers and those affected by this change, which is currently difficult.
S. Golinowska believes that the barriers that stand in the way of changes in health care are conscious and factual - real. In the sphere of consciousness there is:
1. Lack of comprehensive approach to the healthcare system.
2. Simplified diagnosis and numerous gaps in knowledge
about the state of resources in the health care system and the
quality of its management.
3. Selective knowledge about the processes of changing the
healthcare system in other countries, leading to unreliable use of
international comparisons.
4. Shaping the picture of the situation in health care mainly
by the media, which uses selective information, with the dominance
of sensational reports, often unreliable and often shaped by large
interest groups.
5. Phenomena in the sphere of consciousness affect the
formation of real processes and, therefore, lead to a deepening
crisis in the system, which manifests itself:
6. Financial imbalance between funds flowing into the
healthcare system and the costs of its functioning, leading to
systematic indebtedness of health facilities.
7. Imbalance of development between the basic parts of the
health care system: public health, healthcare, rehabilitation and
long-term care.
8. Neglect of basic technical infrastructure and
decapitalization of medical equipment.
9. Wage inequalities, corruption phenomena and outflow of
medical staff abroad.
10. Lack of medical staff: doctors, nurses, midwives, medical
carers, diagnosticians and other medical staff
11. Lack of institutional capacity to make decisions beneficial
from the perspective of the healthcare sector: creation of a
national hospital network, computerization, rational drug policy,
ordering the division of competences. At the same time, taking
organizationally justified decisions as reform activities. These are, for example, actions involving the liquidation or merger of some
institutions, and the creation of others, insufficiently justified and
introduced in advance changes to the criteria for financing health
services, and as a consequence - introducing chaos and anxiety
among patients [5].
In difficult organizational situations, to implement changes in phenomena occurring in the health protection system it is necessary to introduce new solutions that have limited the deepening crisis. The literature on the subject most often draws attention to the need for changes in the financing of healthcare, improvement of change management and implementation of effective organizational and competence solutions. In the sphere of management and organizational-competence solutions, the following are important:
1. Introduction of modern personnel management,
appropriate quantitative and competence selection, staff
training and development,
2. Creating the basis for analyzing the quality of medical
services,
3. Creating information security about resources, services,
patients,
4. Introduction of principles of rational distribution of
facilities and standards of their equipment [6].
When it comes to the financial sphere, the first and essential step to the desired changes is to create an interdisciplinary basket of guaranteed services. Creating such a basket may cause some difficulties (especially in the event of an epidemic crisis). The problem may result from the selection of appropriate criteria for health services. Such benefits should be interdisciplinary: medical, economic and social. In addition, the implementation of these criteria requires numerous and ongoing analyzes of medical effectiveness and cost effectiveness. From the patient’s point of view, the creation of such a basket is associated with the necessity of various payments when using the “non-basket” procedures. In situations where effective treatment is conditioned by the use of above-standard treatment, not covered by basic health insurance, it may turn out that such costs exceed the individual financial capabilities of the patient. To avoid such situations, in many countries the health care system is additionally supported by organizing the entire system of subsidies (co-payment).
The co-payment system takes various forms - small fees that are charged when using benefits, indirect fees, i.e. subsidies for tobacco products or alcohol, up to an increase in the premium for some compulsory insurance, e.g. civil liability of vehicle users. However, the main core are additional health insurance. According to the author, there is also no need to change solutions that work and work well, such as organizational changes in a medical emergency. However, there are also areas that require decisive changes, such as the functioning of hospitals (in the event of an epidemic), the valuation of services, management of health care facilities, computerization (knowledge of resources), quality and availability of health services.
Impact of Individual Stakeholders on the Introduction and Course of Changes in Health Care
All necessary changes in health care should have one main goal: improving the functioning of the system while not compromising its functioning, which will allow to meet the health needs of society. Stakeholders play a leading role in this process, as the type, direction and success of the changes depend on them.
Minister of Health, Health Committee, Parliament
Politicians are the stakeholder group that has the greatest impact on initiating changes in health care, their type and course. The health care system belongs to the public sphere, for which parliament and government are responsible, elected in democratic elections as representatives of society. The system is based on laws, ordinances and other documents adopted by the parliamentary majority. New solutions are most often proposed by the government, MPs or senators, less often by the citizens themselves. Which solutions will be adopted often has no relation to type or quality. The strength of parliament is enormous, because it establishes the law, which is then implemented at all levels in the system. Unfortunately, it happens that the idea for change is unsuccessful, hinders functioning and creates the need for another change. Key decisions are made in parliament that are relevant to all health care stakeholders because they relate to the shape and functioning of the entire system.
The Payer (in Poland is the National Health Fund)
The payer receives money from health insurance premiums paid by patients. It concludes contracts for the provision of health services with entities providing such services and evaluates individual medical procedures. Due to the position of the financial monopolist, he gains great opportunities to influence the functioning of the health care system. Entities providing medical services have little influence on the amount of concluded services or their price. This situation raises many dangerous phenomena, e.g. a hospital pays to treat a patient who is in the ward for more than a certain number of days, or patients with specific diseases whose treatment is highly priced are admitted. By its activities, the payer of medical services does not promote well-managed hospitals, with rational resource management, and high quality of services rendered, which means that weak units sometimes have the same contracts as modern, specialized centers. The payer of medical services, as a central entity under the authority of the state, cannot function independently. This dependence on the government, and at the same time the role it plays, means that it can be included in the bodies with a high potential to influence changes in the health care system.
State Healthcare Institutions
In considering the impact of individual stakeholders on changes in health care, one very important thing should be taken into account, namely the form of ownership of health care providers. Owners, because they can very intensively change health care. In Poland, most hospitals are public facilities. The liquidation, transformation, sale or closure of the facility is the responsibility of the public owner (local governments or the Ministry of Health). Of course, public ownership bodies (appropriate depending on the entity’s reference level) are required to meet the health needs of residents in the area. However, with ever decreasing budget revenues, less money is being allocated to health and the shortage of medical staff, public owners have problems, especially in the event of an epidemic emergency.
The Management of Health Care Institutions
Knowledge, cooperation skills, openness, loyalty to
organizations and employees, creativity, dynamism and activity
of activity, optimism and ability to manage change are the basic
features of the image of a healthcare organization manager. The
structure of these features, and others can be included in their
collection, is not particularly specific if the essence of managerial
work in healthcare is presented in a general way. As in other areas
of managerial activity, there are also consequences for this staff
that appeared along with the systemic change. Managerial work
and management roles are also affected by changes observed from
a global, macro and microeconomic perspective. Understanding
and accepting their presence and taking into account their impact
on management activities are undoubtedly new challenges for the
management of healthcare organizations. Such a challenge, using
M. Crozier’s proposal, is to include in the content a managerial role,
the role of a social innovator who is able to connect people and ideas
and engage them in the processes of solving complex problems of
the reality in which we live [5].
However, special changes in managerial work in healthcare
organizations should be associated with social change. They
broadened the scope of decision-making independence of the
manager and outlined the area of responsibility, which until these
changes was based on different principles and was shaped on a
different basis.
The management of health care institutions plays a much
greater role in implementing and monitoring the course of changes
[E.C. Shapiro]. Managers responsible for implementing new
solutions are required to prepare the ground for changes. This is
primarily related to the preparation of employees: highlighting the
need to introduce changes, presenting the benefits and threats,
gaining acceptance for change. As already mentioned, this is a key
moment for the successful introduction of innovation. Of course, in
small units, the task of the manager is easier. Employees identify
more with the workplace, relations with the manager are often
direct, employees are involved in the decision-making process.
In large entities, especially where employee interests are
defended by trade unions, managers have a difficult task. The
differences also result from the ownership of individual entities.
In public works, managers are subject to the public owner and
act in accordance with the law on public organizations. In private
factories, many changes do not result from the need to apply
the law, but from the owners’ ideas for modernizing the facility,
introducing new services, increasing quality or applying new
technologies. Managers must meet the expectations of owners and
skillfully manage changes.
Private Healthcare Facilities
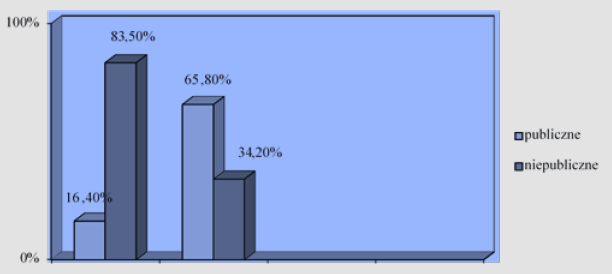
Figure 1: Source: own study based on: Health and health care in 2018 in Polen, Central Statistical Office, Warsaw 2019. Figure 1: Percentage share of public and private entities on the market of health services broken down into hospitals and outpatient care.
Private healthcare facilities are competitors on the market of health services for public entities. These are plants that most often have private owners and private property, but work under a public contract. The growing share of this type of entities in the total number of all health care facilities (Figure 1) may indicate that most changes will be prepared for this type of facilities. New solutions will have to be adapted to the expectations and specifics of the operation of private healthcare facilities. In the event of introducing additional health insurance or separating the payer function, further increase in the number of private entities in other areas of the healthcare system can also be expected.
Mid-Level Medical Staff Managed
Middle management has a special role to play in the process of
change. These personnel are most often described in the literature
as the “executor” of top-level management instructions. R. Kanter
defines the position of middle management in the organization as
“... squeezed between the requirements of strategies beyond their
control and the ambitions of independent thinking employees ...”.
Growing uncertainty means that there must be changes in the area
of activity of employees of “contractors”. It should be noted that
modern organizational concepts limit their activities to key areas.
This view may lead to the conclusion that middle management
can be replaced by technology or computerization. Everything to
“flatten” the organizational structure. This in turn may mean that the
average level of management loses its function. The organizational
structure is flattened, and control functions can be performed, e.g.,
by top management.
E.C. Shapiro believes that management theorists are constantly
“coming up” with new organizational structures. All these proposals
limit the importance of middle management. Are employees losing
importance because the environment is complex? According to
the authors, management theorists - probably yes, according to practitioners - no. The middle management position can be seen as
a simple management process [7]. H. Willke notes that management
concepts refer to planned changes and, as he writes, there is a
“center” capable of observing the results of changes [7,8]. New
strategic initiatives are emerging in planning changes, as W. Bonsiep
and J. Klich notes, through interactive processes in the organization
and up and down hierarchy levels. Therefore, the authors are in
favor of including the average level in activities related to elections
and reorganization activities [9]. They emphasize that the active
inclusion of an average level of the organization in the change
process contributes to:
1. Increasing motivation to change,
2. Obtaining and processing information necessary in the
reorganization process,
3. Average staff is the “link” explaining possible information
disruptions,
4. Enables effective management in large organizations.
The figure below shows the information processing cycle. It
indicates that the amount of information processed at the top
management level prevents the creation of detailed organizational
change plans (Figure 2). This is due to the lack of chance to
implement the given intention without consulting the middle
management level.
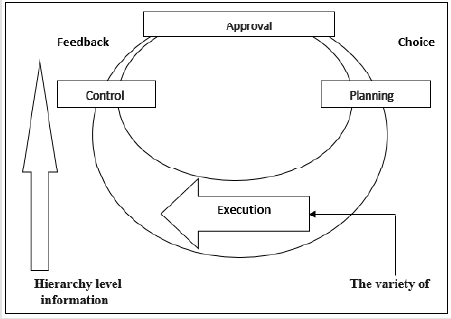
Figure 2: Hierarchically oriented information processing cycle.
Source: W. Bonsiep, J. Klich, Mid-level managers - the barrier to change or a key factor of change, Przegląd Organizacji, No.
2, 2019, p. 20-21.
There are other arguments in favor of recognizing the role of
middle management as an important “actor” of the change process.
Z. Mikołajczyk presents the opinion that there are known cases of
unsuccessful attempts to implement changes without obtaining
mid-level management support [10]. In the opinion of W.D.Guth
and I.C.Macmillan, “... mid-level managers can take over the role
of intermediaries between top-level management and regular
employees [11].
Yet another importance of middle management in change
management results from the participation of each member of
the organization in the efficient and effective implementation of change. Middle management also participates in all phases of the
management process. It should also be remembered that they are
the basic source of innovation in the organization. Recognizing the
significant role of middle management, it is important to include
them in the reorganization process and, above all, provide them
with information so that the planned change can be understood
and accepted. Against this background, the question arises: how
can they object to new solutions? There is no definite answer
to this question. Perhaps it will be brought closer by a field of
knowledge called partner management, whose guiding idea is that
organizations be “closer” to the people who create them.
Patients
The change considered in the subjective area of the organization
focuses primarily on the social aspect. Patients are at the center of
the subjective interest of the change. They are a key factor in the
success of this process. According to Carnall, the effectiveness of
change in 40% depends on solving social problems [12]. People
have to learn the change, take on a new task and then solve it.
Change in the social aspect is primarily its human orientation as
the main focus of interest. Organizations change through people.
After all, people have to assimilate change and take on new tasks.
Therefore, the problem of change should be considered through
the people involved in this process. A. Toffler wrote that “... the
responsibility for change lies with ourselves. We must start with
ourselves, learning not to shut our minds and hearts in advance
of what is new, unexpected and seemingly radical [13]”. In the
literature devoted to the issues of change there is a great variety
in presenting the problem of the patient’s role in the process of
change.
Some authors present the patient’s needs in the process of
change, others talk about the patient’s attitude to change, while
others deal with forms of showing resistance to changes in the
healthcare system. However, it is undoubted that chances for
success in the area of change should be sought in its social resources.
Liz Clarke writes that “a common mistake of many organizations is
underestimating the impact of change on people [14]”. Organization
development is also based on people, because thanks to them the
organization’s resources are multiplied. Each organization through
its social potential is able to efficiently assimilate changes and
organize its activities in such a way as to improve itself. A modern
organization cannot separate its other resources from people
because it would lose its identity and values. Change, and especially
its course, can be a derivative of the appropriate control of the
centers of forces (power) that occur in the organization, as R. L.
Bittel writes [15].
The view of E.M.Rogers may be interesting here, which
distinguished five types of people taking into account the speed
of absorption of changes. They are: innovators, early followers,
early followers, late followers, laggers [16]. Once again, it should
be emphasized that in the subjective aspect of change, one should
pay attention to the fact that the change processes taking place
in organizations are primarily social processes. According to the
American organization and management theoretician Mc Gregor,
people are inherently active and responsible, they want to develop
and manage their own behavior [17-20]. Mc Gregor and his theory
X and theory Y (which became the starting point for the process of
directing through goals) devotes a lot of space to personality and
the role of man. An indispensable condition for the success of the
change is the acceptance of it by the participants and readiness
for behavior conditioning its assimilation. What does the object of
resistance look like to changes? What sources do resistance come
from? What should you do to rationally minimize resistance? How
to make changes so that a person would like to submit to them and
do it voluntarily instead of under duress? We are constantly looking
for answers to these questions.
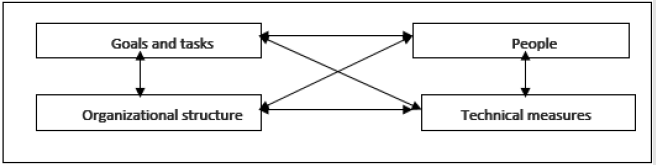
Figure 3: Organizational system by H.J.Leavitta.
Source: H.J.Leavitt: Appelied Organisational Change in Industry. W: Handbook of Organisation. G.March (red.) Chicago 1965, s. 160.
Each changed organization, regardless of the nature of the change or the motive for its creation, creates new working conditions. Almost all modern organizations (teaching, healing, production, administrative, etc.) are treated as complex sociotechnical systems. While the organizational or technical condition can be adapted to changes in the environment, for example by reorganizing the process or transferring technology, people are not easily modified. H.J. Leavitt’s model is the most general and also the most universal organization model in which people occupy high rank. The essence of his model are the feedback between people, the goals of the organization, the organizational structure and technical means (Figure 3). People create their future image through their influence on individual elements of the organization. Man influences technical means deciding about the scope of their use. In turn, technical means force people to learn new skills in their use. The human impact on the organizational structure, on the other hand, determines the formal solutions adopted in a specific organization and informal solutions, which in an ad hoc manner and depending on the need for rapid change condition some decisionmaking powers.
The organizational structure shapes social relations, organizational roles of individual members of the organization. Against this background, we are dealing with a large human relationship with the change management process. It is worth emphasizing at this point that the starting point in these considerations is a single person or group of people who influence the success of reorganization plans Summing up the considerations of the participation of stakeholders in the process of changes in health care organizations, it can be said that their behavior in the face of changes is extremely important. These behaviors should be oriented towards efficient change management. Today (especially in the event of an epidemic crisis), as well as in the future, stakeholders should effectively participate in the process of change, prepare changes to create a good image of change. Building change requires the participation of individual stakeholders at every stage of this process. The success of changes depends above all on promoting a new reality, sharing knowledge, as well as creating mutual trust in the constantly changing face of healthcare organizations.
Conclusions
Bearing the above in mind, the author comes to the following conclusions:
1. There are many stakeholders in the healthcare system.
Their significance depends on many factors: power, economic
resources, the roles they play, and the impact they have on the
functioning of health care.
2. All stakeholders have a very important goal to achieve
- ensuring health security for the public. Regardless of whether
their impact on change is large or not, it is important for everyone
to make efforts to create an ever better functioning health care
system, a system that everyone can afford.
3. The changing health protection system must cultivate
“social capital” in which man is the highest value. Based on the
words of D. Cohen and L. Prusak, it can be added to the above
statement that “management in the organization of health care
is not only taking risks, but caring for human capital and social
capital”.
4. Managers of healthcare organizations know that in
order to make effective decisions about implementing changes,
patients must be in the foreground. Patients constitute “capital”
- an intangible asset of a healthcare organization. The position of man in the entire changing economic process of our millennium has
been recognized. Assumptions of P.M.Senge in ‘The Tifth Discipline.
Although the Art. And Practice of The Learning Organization refer
to the concept of the so-called a learning organization, but in order
to be able to fulfill its most ambitious aspirations and changes,
the organization must implement, among others, the so-called
thought models - based on discovering the real reality about the
organization and the people creating them.
References
- Friedman AL, Miles S (2016) Stakeholders Theory and Practice, University Press Oxford, New York.
- Stoner J, Freeman R, Gilbert D (2018) Kierowanie, PolskieWydawnictwoEkonomiczne, Warszawa.
- Carneal CA (2016) Managing, Change in Organizations, University Press Oxford, New York, USA.
- Robbins S (2012) Zachowania w organizacjach, PolskieWydawnictwoEkonomiczne, Warszawa.
- Crozier M, Friedbarg E (1982) Człowieki system. Ograniczeniadziałaniazespołowego, PWE, Warszawa.
- Flora C (2014) Building Social Capital: The Importance of Entrepreneurial Social Infrastructure. www.ag.iastate.edu.
- Shapiro EC (2015)Trendsurfen in der Chefetage – Unternehmenshifrungjenseits der Managementmodem, Frankfurt.
- Willke H (2015) Systemtheorie – 3Steuerungstheorie, Stuttgart.
- Bonsiep W, Klich J (2019) Mid-level managers - the barrier to change or a key factor of change, PrzeglądOrganizacji, No. 2, pp. 20-21.
- Mikołajczyk Z (1999) Kadrakierowniczapolskichprzedsiębiorstwpaństwowych w warunkachzmiansystemugospodarczego, WydawnictwoUniwersytetuŁódzkiego, Łódź.
- Golinowska S (2004) Pożądanekierunkizmianysystemuochronyzdrowia w Polsce. Międzyracjonowaniemiracjonalizacją, Centrum AnalizSpołeczno-Ekonomicznych, Warszawa.
- Golinowska S, Boni M (2006) Nowedylematypolitykispołecznej, Centrum AnalizSpołeczno-Ekonomicznych, Warszawa.
- Halal, William E (1996) The New Management. Democracy and Enterprise are Transforming Organizations, Berrett – Koehler, San Francisco.
- Herrera J (2011) Participatory Management, Teamwork and leadership. Key Requirements for the Success of Organizations in the Twenty-first Centur. https://www.ohrd.wisc.edu/home/Portals /0/ Week1Partcipatory ManagementTeamworkLeadership-Herrera.pdf (12.02.2020).
- Hodgkinson A (1999) Employee Involvement and Participation in the Organizational Change Decision: Illawarra and Australian Patterns, Working Paper 99-7, Department of Economics, University of Wollongong.
- Rogers EM (2013) Diffusion of Innovations, New York.
- Kohen M, Prusak L (2015) In Good Company: How Social Capital Makes Organizations Work, Harvard Business School Press”, Boston.
- Kanter R (2016) The reshaping of middle Management, [w:]Management Review.
- Lessem R (2016) Global Management Principles, Prentice – Hall, New York.
- Leavitt HJ (1965) AppeliedOrganisational Change in Industry. W: Handbook of Organization. G March (red.) Chicago.
