 Case Report
Case ReportAbstract
This case report details Joubert syndrome (JS), first described by Marie Joubert in 1968, is a congenital anomaly characterized by episodic hyperpnea, abnormal eye movement, ataxia, intellectual disability and typical “molar tooth sign” in Magnetic Resonance Imaging (MRI) findings. There are only twelve papers which explain about the congenital deformities of the extremities which are mostly postaxial polydactyly of the hands and preaxial polydactyly of the feet. Our patient had bilateral polysyndactyly of the ring finger from the middle phalanx to distal phalanx in the right hand and from the metacarpal bone to the distal phalanx on the left and polydactyly from the proximal phalanx to the distal phalanx of the right great toe. In comparison with previous reports, the morbidity rate of polydactyly is 30.19%.
Introduction
Joubert syndrome (JS), first described by Marie Joubert in 1968, is a congenital anomaly characterized by episodic hyperpnea, abnormal eye movement, ataxia and intellectual disability. Congenital deformities of the extremities are mostly postaxial polydactyly of the hands and preaxial polydactyly of the feet. Typically, a y-shaped metacarpal bone between the middle and ring finger is seen on x-ray. Our patient had bilateral polydactyly of the ring finger from middle phalanx to distal phalanx in the right hand and from the metacarpal bone to the distal phalanx on the left and polysyndactyly from the proximal phalanx to the distal phalanx of the right great toe. In this study we describe this atypical our atypical case in comparison with previous reports.
Case Report
The patient was a male infant born with a caesarean section with a weight of 3278g at 38weeks and 3days gestation. At birth the Apger score was 9points/1min, 10points/5mins then he was sent to our hospital because of the screening about malformations. Examination revealed abnormal eye movement, tongue tumor (Figure 1), and bilateral polydactyly of the ring fingers (Figure 2), and poly syndactyly of the right great toe (Figure 3). Magnetic Resonance Imaging (MRI) findings shows typical “molar tooth sign” (Figure 4). He shows hypotonia and developmental delays, but He hasn’t retinal renal, hepatic, orofacial defect (Figure 5). Our comprehends literature search of Pubmed on congenital hand anomalies in Joubert syndrome revealed that from 1968 to 2017.
Results
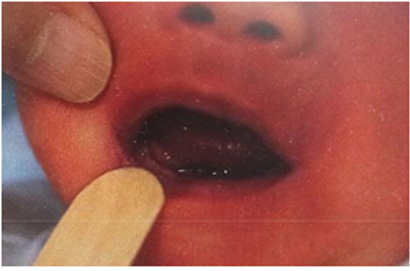
Figure 1: Tongue tumor at the right bottom.

Figure 2: The phenotype appearance of his right hand and left hand.

Figure 3: The phenotype appearance of the right foot and left foot.
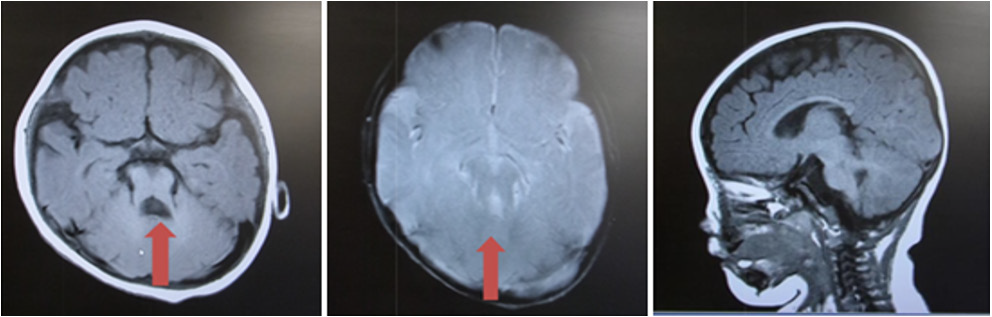
Figure 4: MRI findings axial slice of T1,T2 weighted image shows typical Molar Tooth Sign(red arrow) sagittal image shows the thickening of the superior cerebellar peduncle.
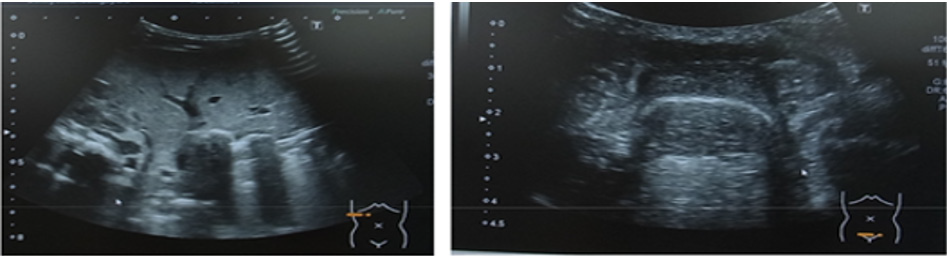
Figure 5: Urtrasonography: There were no renal, hepatic defects.

Figure 6: The operation view for the left hand.

Figure 7: The operation view for the left hand.
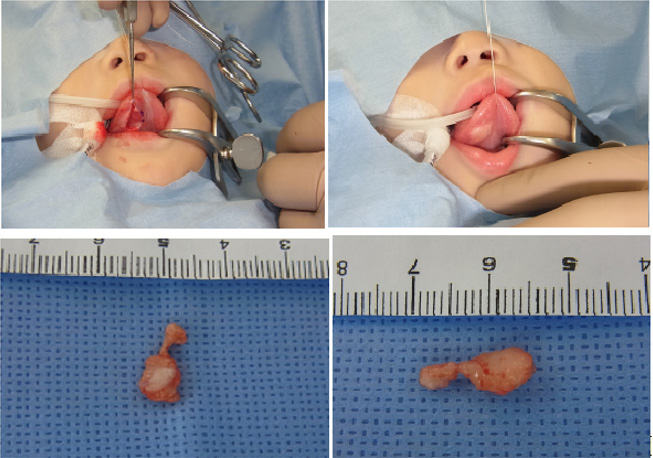
Figure 8: The operation view of the tongue tumor.
Our case was diagnosed as Joubert syndrome with orofaciaodigital defects. For right hand and right foot, the operation was performed first, 3months later it was done for the left hand. For his left polysyndactyly we selected the Bilhaut procedure because two fingers of polydactyly were both very small (Figure 6). The tongue tumor was resected at the same time (Figures 7 & 8). The patholog ical findings were lipoma not hamartoma (Figures 9 & 10). 1 year after surgery, the PIP joint of the right ring finger showed the limitation of the range of motion. The rehabilitation was put for his disability of movement by the occupational therapist. He can use both hands actively and grasp the small toys using all fingers. He has hypotonia and developing delays, so he can’t sit alone at the age of 1 year and 11months. There is no sign of respiratory and renal functional problem.
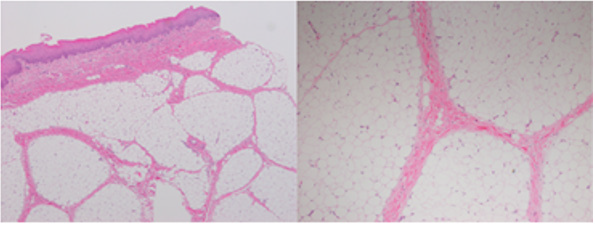
Figure 9: 9: H-E stain lipoma x40 x100.

Figure 10: 1year after operation the only DIP joint of the left ring finger had limitation of the active and passive range of motion.
Discussion

Table 1: The classification of Joubert syndrome.
The incidence of Joubert syndrome is between 1/80.000 and 1/100.000 live births. Several candidate genes were published such as AHI1, CC2D2A, CEP290, ARL13B, C50RF42, TCTN2 in Joubert syndrome with orofaciodigital defect, but we have not done genetic testing yet because of his parent’s issue. Joubert syndrome is classified into 6 types (Table 1). Since1968 to 2017 twelve reports explained about hand condition in detail (Table 2). The average of morbidity of polydactyly is 30.19% (8-100%). Varadi first discribed about the hand phenotype of Joubert syndrome in 1980. His case was the syndactyly between middle and ring finger. Polydactyly is seen in 8-19% of JS, occurs between the central digits and the typical phenotype is Y-shaped metacarpal bone. In the literature, preaxial polydactyly is major in the foot but postaxial polydactyly is major in the hand. Dohforerty described that polydactyly is not functionally signify, and surgical correction is at the discretion of the patient/family. Wentzensen explained about the one case who was gotten the operation for cleft palate and hamartoma of the tongue but didn’t described about the operation for the extremities. The reason is that JS couldn’t get the operation because Saraiva told 11 of 87 children died within the first year of life. Saravia Silverstein and Steinlin explained the survival of JS without renal problem exceeded that of patients with renal problem. From this fact, we actively have to plan the operation for extremities of the patients without renal problem. Even patients with kidney problems should rather consider the operation for extremities in order to the development of extremities.

Table 2:
Conclusion
A case of Joubert syndrome with orofaciodigital disorder was shown. Over 200 papers were published about Joubert syndrome, but there are only 12 papers described about extremities. Most phenotype pattern of Joubert syndrome is postaxial polydactyly, but our case shows preaxial polydactyly of the right toe and polydactyly of bilateral ring fingers. Considering the associated intellectual disability, it is important to make use of the fingers easier by surgery. Careful observation of the development and guidance for the patient and the family are also important because there is a possibility of acquiring more abilities.
References
- Varadi V, Szabó L, Papp Z (1980) Syndrome of polydactyly, cleft lip/palate or lingual lump, and psychomotor retardation in endogamyic gypsies. Journal of Medical Genetics 17(2): 119-122.
- Pellegrino JE, Lensch MW, Muenke M, Chance PF (1997) Clinical and molecular analysis in Joubert syndrome. Am J Med Genet 72(1): 59-62.
- Kumandas S, Akcakus M, Coskun A, Gumus H (2004) Joubert syndrome: review and report of seven new cases. Eur J Neurol 11(8): 505-510.
- Parisi M (2009) A Clinical and molecular feature of Joubert syndrome and related disorders. Am J Med Genet C Semin Med Genet 151C(4): 326-340.
- Doherty D (2009) Joubert syndrome: insights into brain development, cilium biology, and complex disease. Semin Pediatr Neurol 16(3): 143-154.
- Chih Ping Chen, Yi Ning Su, Jon Kway Huang, Yu Peng Liu (2010) Fetal Magnetic Resonance Imaging Demonstration of Central Nervous System Abnormalities and Polydactyly Associated with Joubert Syndrome Taiwan Jobstet Gynecol 49(2): 243-246.
- Huppke P, Wegener E, Böhrer Rabel H, Bolz HJ, Zoll B, et al. (2015) Tectonic gene mutations in patients with Joubert syndrome. Eur J Hum Genet 23(5): 616-620.
- Wenzensen IM, Jennifer J Johnston, John H Patton, John M Graham (2016) Exome sequencing identifies a mutation in OFD1 in a h complex polydactyly. Human Genome Variation 3.
- Bachmann Gagesuu R, Dempsey JC, Phelps IG, O Roak BJ, Knutzen DM, et al. (2015) Joubert syndrome: a model for untangling recessive disorders with extreme genetic heterogeneity. j med genet 52(8): 514-522.
- Srour M, Hamdan FF, McKnight D, Davis E, Mandel H, et al. (2015) Joubert Syndrome in French Canadians and Identification of Mutations in CEP104. The American Journal of Human Genetics 97(5): 744-753.
- Kroes HY, Monroe GR, van der Zwaag B, Duran KJ, de Kovel CG, et al. (2016) Joubert syndrome: genotyping a Northern European patient cohort. European Journal of Human Genetics 24(2): 214-220.
- Johnston JJ, Lee C, Wentzensen IM, Parisi MA, Crenshaw MM, et al. (2017) Compound heterozygous alterations in intraflagellar transport protein CLUAP1 in a child with a novel Joubert and oral-facial-digital overlap syndrome. Cold Spring Harb Mol Case Stud 3(4): a001321.
