 Short Communication
Short CommunicationShort Communication
represent frequent conditions in clinical practice. As objectively measurable physiological and structural abnormalities for GI complains are often absent in the patients, functional abdominal symptoms may in fact make up for 30 to 50% of all cases in gastroenterology [1,2]. The importance of these complaints is illustrated by the fact that 45% of the American population [3] regularly consume proton inhibitors, often without any significant efficacy. A variety of attempts to objectify these conditions were undertaken, including manometry, measurements of acidity, electromyography, and scintigraphic studies of stomach emptying. All of these may be considered as largely influenced by the vegetative nervous system. The vegetative origin of such complaints is further supported by the fact that visceral hypersensitivity to mechanical distension [4-6] and psychological and psychiatric conditions like anxiety and depression are frequent features of upper abdominal syndromes [1]. In fact, several experimental studies link stress and depression to changes in sensory and motor gastrointestinal function [1] which also is largely regulated by the enteric nervous system as part of the autonomous nervous mechanisms.
It is comparatively difficult to induce specific functional changes in the autonomous regulation of the related stomach and bowel movements by means of conventional medicine. Therefore, we were interested in searching for a method to differentiate individual upper abdominal syndromes for further vegetative reflex treatment. We correlated reflex treatments by acupoints with specific hyperalgesic pressure points in the abdomen. These reflex points were taken a modern rational concept of Chinese Medicine [7-9], which is able to translate Chinese medical theory into the language of Western physiology [10,11]. This contemporary understanding of reflex point selection had already enabled us in prior doubleblinded clinical acupuncture studies to objectively detect reliable clinical effects [12-16]. We were therefore able to link the Western teaching of hyperalgesia with the treatment by acupuncture points, resulting in immediate reduction of hyperalgesic points in the upper abdomen. Some of the most frequently affected hyperalgesic points were then named G1 to G5. They were linked to western abdominal anatomy and therefore upper abdominal physiology. The clinical efficacy of the five related reflexologic acupoint interventions was clinically so impressive that they were taken up in the curriculum of the first master’s degree of Chinese Medicine in Europe at Porto University, and are rapidly spreading within the related medical communities ever since. We were therefore interested to see what objectively is known about this pressure point-based reflex therapy and performed this literature review to look for the existing evidence of effects and mechanisms (Figure 1).
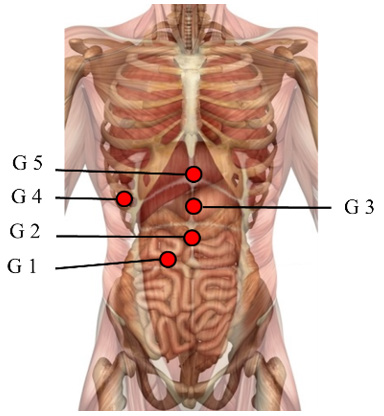
Figure 1: Location of the points G1 – G5. Note that these pressure-sensitive points are located intra-abdominally and project to the skin as shown in the picture.
Methods
We performed a literature search in pubmed and scopus with the following keywords: G1, G2, G3, G4, functional abdominal complaints and acupuncture, functional abdominal complaints and reflex diagnosis, and functional abdominal syndromes and pressure points. None of these would reveal any research on that topic. We would then enlarge our search by the inclusion of textbooks, scripts and master theses available and summarized the G1-G5 methodology and first evidence of its mechanisms as follows:
Results
Although the usage of G1-G5 methodology is already spread widely within the medical community in Germany and Southern Europe, no conclusive research papers were listed in pubmed and scopus. Detection of the respective syndromes is performed by comparing the pressure sensitivity in the points G1 to G5 by simple comparison of pressure tolerance of the points. Note that these points are no acupoints like the alarm or mu points which are located in the skin level, but that they are located in the intraabdominal organs Sphincter,Oddi, Pylorus, corpus stomachi, and on the stomach entry (below the xiphoid process). A first information on the distribution of theses syndromes may be roughly taken from a study [17], in which 30 otherwise healthy volunteers were examined. Twelve individuals showed G1 (40 %), four individuals with G2 (13,3 %), three individuals with G3 (10 %), three individuals with G4 (10 %) and eight individuals with G5 (26,6 %).
G1
Corresponds to the duodenal loop and is precisely located on the sphincter Oddi, the small smooth muscle which controls bile excretion. The syndrome is diagnosed when G1 is comparatively the most hyperalgesic point of the five G points in question. In an experiment [18], pain evoked by a defined pressure on the G1 point decreased by 81.8% (p = 0.002), indicating that hyperalgesia could be reduced (points GB 39, 26, 41, Li 3 and S 44) in a sample of 33 otherwise healthy volunteers. Also, electromyography was performed but stomach movements showed no difference before and after acupuncture.
G2 Syndrome
This syndrome is diagnosed when the point above the pylorus (Rs 10) is the most pressure-sensitive of all G points. N=20 otherwise healthy volunteers with G1 syndrome were treated by the points Rs 10, S 44, S 25 which reduced the pain in the hyperalgesic region of the pylorus statistically significantly (30.68%), whereas control points did not have this effect The points Bl 66, Rs 15 and an extra point did not significantly change pain. Furthermore, gastric contractility in EMG increased, whereas pyloric pain decreased, presumably indicating release of pyloric tonus and onset of gastric emptying [19].
G3 Syndrome
This syndrome is diagnosed when the corpus of the stomach located under the point Rs 12 clinically shows the comparatively highest-pressure sensitivity of all G points. According to the transcription of Chinese medical theories, this would be associated with impairment of gastric emptying, while pancreatic exocrine activity may be diminished. In the literature, we did not find any further data on that.
G4 Syndrome
This syndrome is diagnosed when the region of the gallbladder is pressure sensitive. In this case, treatment of the gallbladder alarm point (mu point) is indicated and in practice is believed to be effective. However, we found no data on that.
G5 Syndrome
This syndrome is diagnosed when the region of the xiphoid process is most sensitive. This is the region where the oesophagus passes the diaphragm. Frequent diagnoses in Western medicine are gastro-oesophageal reflux with heartburn. In the literature quoted, there was no indication of any measurements on that.
Discussion and Conclusion
The bottom line is that this is a promising field of research which should be followed up. We suggest that a double-blinded study is performed according to the so-called Heidelberg doubleblinding assay. For this purpose, patients with upper abdominal complaints should be screened for G2 syndrome and a two-armed double-blinded study be performed using pressure tolerance on the G2 point and electromyography as main parameters.
References
- (2012) International Association for the Study of Pain. Global year against visceral pain, Oct 2012 - Oct 2013. Painful Functional Bowel Disorders: Psychological Factors. IASP.
- Takahashi T (2011) Mechanism of Acupuncture on Neuromodulation in the Gut-A Review. Neuromodulation: Technology at the Neural Interface 14: 8-12.
- Carvalho Antonio (2010) Determinar a eficácia de adicionar Acupuntura verso dobrar dose de IBP em doentes com DRGE que falharam tratamento sintomático com dosagem standard de IBP uma vez por dia. Dissertação de mestrado em Medicina Tradicional Chinesa. ICBAS-UP.
- Mertz H, Fullerton S, Naliboff B, Mayer EA (1998) Symptoms and visceral perception in severe functional and organic dyspepsia. Gut 42(6): 814-822.
- Tack J, Caenepeel P, Fischler B, Piessevaux H, Janssens J (2001) Symptoms associated with hypersensitivity to gastric distention in functional dyspepsia. Gastroenterology 121(3): 526-535.
- Vandenberghe J, Vos R, Persoons P, Demyttenaere K, Janssens J, et al. (2005) Dyspeptic patients with visceral hypersensitivity: sensitisation of pain specific or multimodal pathways? Gut 54(7): 914-919.
- Greten HJ (2017) Kursbuch Traditionelle Chinesische Medizin (Textbook of TCM) (3rd). Thieme, Stuttgart - New York, USA. pp. 692.
- Greten HJ (2017) Understanding TCM - Fundamentals of Chinese Medicine - Part I: Basic Clinical Sciences (8th ). Heidelberg School Editions, Heidelberg, Germany.
- Greten HJ (2017) Understanding TCM - Fundamentals of Chinese Medicine - Part II: Advanced Clinical Sciences (8th). Heidelberg School Editions, Heidelberg, Germany.
- Greten HJ (2017) Understanding TCM - The Fundamentals of Chinese Medicine - Part III: Foraminology. Heidelberg School Editions, Heidelberg, Germany.
- Greten HJ (2017) Clinical Subjects - Vol I: Gastroenterology (6th). Heidelberg School Edition, Germany.
- Hauer K, Wendt I, Schwenk M, Rohr C, Oster P, et al. (2011) Stimulation of Acupoint St 34 Acutely Improves Gait Performance in Geriatric Patients During Rehabilitation: A Randomized Controlled Trial. Arch Phys Med Rehabil 92(1): 7-14.
- Karner M, Brazkiewicz F, Remppis A, Fischer J, Gerlach O, et al. (2013) Objectifying specific and non-specific effects of acupuncture: A double-blinded, randomised trial in osteoarthritis of the knee. Evid Based Complement Alternat Med.
- Duarte Alcino (2012) Efeitos agudos da acupuntura na dor lombar crónica estudo prospetivo randomizado, controlado e duplo-cego. Dissertação de tese de mestrado em Medicina Tradicional Chinesa. ICBAS-UP.
- Seca S, Kirch S, Cabrita AS, Greten HJ (2016) Evaluation of the effect of acupuncture on hand pain, functional deficits and health-related quality of life in patients with rheumatoid arthritis - A study protocol for a multicenter, double-blind, randomized clinical trial. J Integr Med 14(3): 219-227.
- Seca S, Patrício M, Kirch S, Franconi G, Cabrita AS, et al. (2018) Effectiveness of acupuncture on pain, functional disability and quality of life on rheumatoid arthritis of the hand - Results of a double-blind randomized clinical trial. J Altern Complement Med 25(1): 86-97.
- Ferreira Vera (2019) Impulsividade: Ativação neurovegetativa da emoção e sua relação com o aparelho gastrointestinal. Estudo observacional analítico transversal. Dissertação de mestrado em Medicina Tradicional Chinesa. ICBAS-UP.
- Marques André (2019) Efeito da acupuntura na atividade mioelétrica abdominal. Estudo preliminar Prospectivo e Randomizado. Disssertação de mestrado em Medicina Tradicional Chinesa. ICBAS-UP.
- Martins Susana (2015) Comparação de duas estratégias de acupuntura na atividade mioelétrica do estô Estudo Preliminar, Prospetivo, Randomizado e Cego. Dissertação de mestrado em Medicina Tradicional Chinesa. ICBAS-UP.
