 Case Report
Case ReportAbstract
Carcinoma of the nasal cavity and paranasal sinuses is a rare malignancy. Due to non-specific symptoms, up to 75% of patients with paranasal sinus cancer present with advanced disease, when the tumor affects different vital structures. This circumstance determines a poor prognosis and low survival rate. We report the case of the patient who presented with stage 3 maxillary sinus cancer and underwent three-modality therapy: induction chemotherapy, radiotherapy and surgery. The patient’s follow up period is 7 years and she remain disease-free.
Introduction
Carcinoma of the nasal cavity and paranasal sinuses is a rare malignancy. The incidence ranges between 0.2% and 1.4% of all neoplasms and about 3% among tumors of the upper respiratory tract [1,2]. In Russia in 2018 the incidence rate was 0.67 per 100.000 people. Notably, over the past 10 years there has been an increase in the incidence of almost 8% [3]. For a long time, a carcinoma of this localization can manifest as a nonspecific disease, or even be asymptomatic [4]. This is one of the reasons late patients seek medical attention. Currently, up to 75% of these patients present with advanced stages, when the tumor affects different vital structures such as the orbit, zygomatic bone, pterygopalatine and temporal fossa, cranial cavity or extends to the opposite side [5,6]. The main method of treatment for this disease is surgery, followed by radiotherapy. Such treatment allows for an overall 5-year survival of more than 60% of patients with a localized tumor, decreasing to 35% in stage IV disease [7]. Due to the advanced stages at which paranasal sinus malignancies are presented a lot of patients are subjected to palliative treatment with use of chemotherapy [8]. Thus, considering unsatisfactory cosmetic results after surgical treatment, relatively low survival rates, and difficulties in performing radiotherapy, the use of induction chemotherapy seems to be a reasonable area for investigation [9].
Case
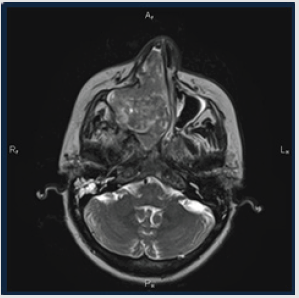
Figure 1: (left) – CT paranasal sinuses before treatment.
A 45-year-old female presented with nasal obstruction and bleeding from right nasal cavity with 6-month duration. The MRI scan showed the tumor in the right maxillary sinus (5.1x8.1x4.4cm). It destroyed the medial wall, extended to the right half of the nasal cavity, pushed the nasal septum with signs of its destruction and subtotal obstructed the left nasal cavity. It infiltrated the hard palate, the alveolar process of the lower jaw at the level of premolars and molars, spread to the cells of the ethmoid labyrinth (more on the right). The tumor also extended to the right pterygopalatine fossa involving the pterygoid muscles (Figure 1). The biopsy from nasal mass was reported as a low-grade non-keratinizing squamous cell carcinoma with extensive necrosis zone.
Treatment
From 03/07/12 to 10/27/12 the patient received 6 courses of Chemotherapy (CT) according to the TPF regimen (cisplatin 75 mg/m2 for day 1 + docetaxel 75 mg/m2 day 1 and 5-fluorouracil 1000 mg/m2/day for 96 hours infusion). After each course of CT, prophylactic administration of Colony-Stimulating Factors (CSFs) was carried out. According to the control examination, a partial response of the tumor was recorded. MRI on 11/01/12: the tumor remained on the inferior wall of the right maxillary sinus with infiltration of the hard palate and alveolar process of the lower jaw at the level of premolars and molars, the general linear dimensions of the tumor was 1.7x1.8 cm, length up to 2.0 cm. Medium and the upper parts of the right maxillary sinus were free from tumor mass. The medial wall of the right maxillary sinus was destroyed; however, the nasal cavity was free (Figure 2) Patient further received conformal radiotherapy from 11/26/12 to 12/26/12 with unconventional fractionation: 3 sessions of 4 Gy, followed by sessions of 2 Gy (total dose is 50 Gy) (Figure 3).
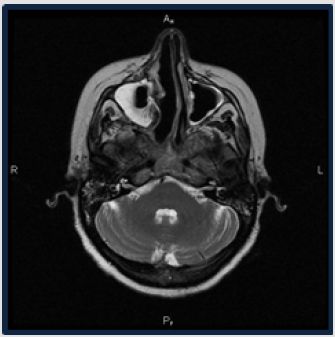
Figure 2: (right) – CT paranasal sinuses after treatment.

Figure 3: Conformal radiotherapy plan.
Patient further received conformal radiotherapy from 11/26/12 to 12/26/12 with unconventional fractionation: 3 sessions of 4 Gy, followed by sessions of 2 Gy (total dose is 50 Gy) (Figure 4). In January 2013, there was resection of the upper jaw on the right with Radiofrequency Ablation (RFA). Despite the fact that the dose of radiotherapy was only 50 Gy, pathologically complete response was achieved. At the time of the case report (February 2020), the patient is still on the regular follow up and remains disease-free for more than 7 years duration. The patient’s appearance is in the photo (Figure 4).

Figure 4: The patient’s appearance after treatment.
References
- Porceddu S, Martin J (2004) Paranasal sinus tumors: Peter MacCallum Cancer Institute experience. Head Neck 26(4): 322-3
- Turner JH, Reh DD (2012) Incidence and survival in patients with sinonasal cancer: A historical analysis of population-based data. Head Neck 34(6): 877-88
- Ansa B, Goodman M, Ward K (2013) Paranasal sinus squamous cell carcinoma incidence and survival based on Surveillance, Epidemiology, and End Results data, 1973 to 2009. Cancer 119(14): 2602-26
- Allen M Chen (2010) Cancer of the Nasal Cavity and Paranasal Sinuses. Leibel and Phillips Textbook of Radiation Oncology (3rd Edn.), 30: 438-451.
- William M Mendenhall, Robert J (2009) Carcinoma of the Nasal Cavity and Paranasal Sinuses. The Laryngoscope 119(5): 899-906.
- Mahalingappa YB, Khalil HS (2014) Sinonasal malignancy: Presentation and outcomes. The Journal of Laryngology & Otology 128(7): 654-65
- Gore MR (2018) Survival in sinonasal and middle ear malignancies: A population-based study using the SEER 1973-2015 database. BMC Ear Nose Throat Disord 18:
- Patil VM, Noronh V, Joshi A, Karpe A, Talreja V, et al. (2016) Metronomic palliative chemotherapy in maxillary sinus tumor. South Asian J Cancer 5(2): 56-5
- Ock CY, Keam B, Kim TM, Han DH, Won TB, et al. (2016) Induction chemotherapy in head and neck squamous cell carcinoma of the paranasal sinus and nasal cavity: A role in organ preservation. Korean J Intern Med 31(3): 570-57
