 Research Article
Research ArticleAbstract
Objective: During craniotomy for the cerebellopontine angle (CPA) lesion using the typical retrosigmoid approach, exact exposure of the margin of the venous sinuses remains an essential but risky step. This study aimed to establish an accurate and practical method for identifying the individualized relationship between the location of the asterion and the transverse and sigmoid sinuses junction (TSSJ).
Methods: We utilized preoperative images including computer tomography (CT) and/or magnetic resonance imaging (MRI) combined with intraoperative anatomical landmarks to determine the exact position of the sigmoid sinus and TSSJ. MRI T1 sequences with gadolinium and/or the CT bone window were used for the distance relationship of the asterion to sigmoid sinus.
Results: In all 94 cases, preoperative images identifying the distance from the asterion to sigmoid sinus at the transverse sinuse level, enabled the intraoperative location of the TSSJ, with an accuracy flaw below 2 millimetre (mm). Just one case had a laceration of the sigmoid sinus during the craniotomy.
Conclusion: Usage of preoperative image combined with intraoperative anatomical landmarks is a reliable method in the localization of the TSSJ for retrosigmoid craniotomy and thereby avoiding unnecessary sinus injury and bone defect. In addition, the method proved to be fast and accurate sinuses exposure.
Abbreviations: TS: Transverse Sinus; SS: Sigmoid Sinus; CPA: Cerebellopontine Angle; TSSJ: Transverse and Sigmoid Sinuses Junction; VS: Vestibular Schwannomas; CT: Computer Tomography; MRI: Magnetic Resonance Imaging
Introduction
The retrosigmoid approach is one of the commonly used procedures for the CPA surgery [1]. Exposure of the sigmoid sinus and TSSJ remains a pivotal but advent neurosurgical practice [2,3]. During the course of exposure of venous sinuses, making the venous sinuses visualized is essential for the localization of the burr-hole dot on the TSSJ, avoiding hazardous step into the venous sinuses and limitation of the size of the bony opening. We report a prospective study of 94 retrosigmoid craniotomies. This image-guided anatomic study revealed the exact position relationship between the asterion and the TSSJ in every patient. Preoperative CT and MRI data from 94 patients were studied. Study of two sides yielded 188 sides. Distance measurement from the asterion to the posterior edge of the TSSJ on preoperative CT or MRI was performed in preoperative image system and relations of the external landmarks with the TSSJ during surgery was studied according to preoperative image measurement. The distance from the asterion to the TSSJ was variable in different patients. The projection of transverse sinus roughly overlapped with the asterion. The beeline from the asterion to the spot, that is body surface projection of the posterior margin of the TSSJ, was measured on preoperative image. An exact burrhole dot just placed in the front of asterion is appropriate for both avoiding inadvertent entry into the sinus and limiting the size of the craniotomy.
Patients and Methods
From February 2008 to November 2019, 94 patients who underwent retrosigmoid craniotomies for removal of vestibular schwannoma (VS) were enrolled in our series. Of these patients, 38 were male while 56 were female. The mean age of male patients was 46.26 ± 14.60 years while the mean age of female patients was 47.96 ± 11.84 years. Study of two sides was 188 sides. The following structures were identified on each side: the lambdoid suture, parietomastoid suture, asterion, inion, occipitalmastoid suture, posterior zygoma root and mastoid process. For surgical planning, thin-slice, 1-mm-thick CT and enhanced CT venous images (Philips, brilliance, 6-slice CT machine) were performed and reconstructed by volume-rendering methods. Once generated, structure meshes could be visualized and manipulated in a three-dimension (3D) viewing window and by image editor. Using basic cutting and cropping tools on anatomic structures of interest, only ipsilateral 3D skull bases with lesions were left. The three-dimensional reconstructed transverse and sigmoid sinuses and its projection on the ipsilateral 3D skull base were represented in the visualization mode (Figure 1A). After identification of the key structures, the distance was measured: the asterion to the body surface projection of posterior edge of sulci for transverse and sigmoid sinuses on the inner surface. The distance between TSSJ and occipitomastoid suture is reflected as red line (Figure 1B).
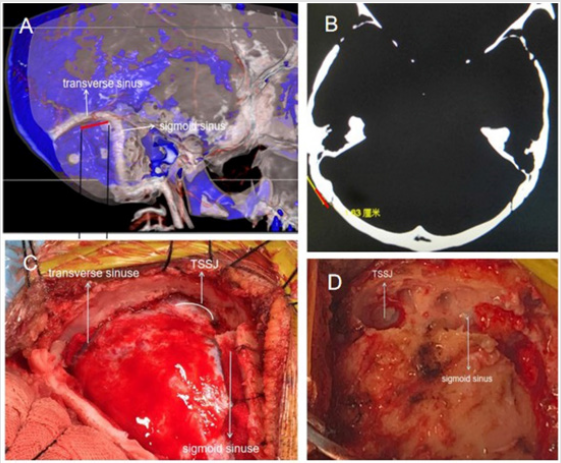
Figure 1: Three-dimensional reconstructed transverse and sigmoid sinuses and its projection on the skull (right). A. The red line is defined as the distance from the asterion to the body surface projection of posteroinferior edge of sulci for transverse and sigmoid sinuses on the inner surface. B. The red line stands for the shortest distance from the occipitalmastoid suture to the posterior margin of sigmoid sinus groove on the bone window of craniocerebral CT. C. Intraoperative photo shows that the burr-hole exactly exposes the margin of TSSJ and the sigmoid sinus. D. Intraoperative photo shows that the exposed margin of TSSJ, sigmoid sinus and transverse sinus.
A linear skin incision along venous sinuses was drawn, with rough 7-centimeter length. After the bone exposure, anatomical structures within the district can be discriminated and the umbriferous position of the TSSJ can be determined on the base of preoperative image-guided individualized anatomical localization. The asterion and the body surface projection of posterior edge of TSSJ position were ascertained on the bone as a landmark for the burr hole dot and craniotomy. The shortest distance between these two dots (asterion and projective TSSJ) was measured in millimeters. The burr hole was placed medially and inferiorly at the location of the TSSJ to avoid undesired sinus exposure (Figure 1C). After craniotomy, the real position of the medial and inferior margin of the TSSJ, sigmoid sinus and transverse sinus was limpidly exposed (Figure 1D). Continuous variables were shown as mean ± standard deviation (SD). Categorical variables were shown as counts and percentages. We applied independent-samples T test to compare the differences of the distance relationship between genders and sides. Scatter plot and Pearson product-moment correlation coefficient were utilized to explore the linear correlation between distance and age. A two‑tailed P < 0.05 was considered statistically significant. All data were analyzed with IBM® SPSS® Statistics Version 20.
Results
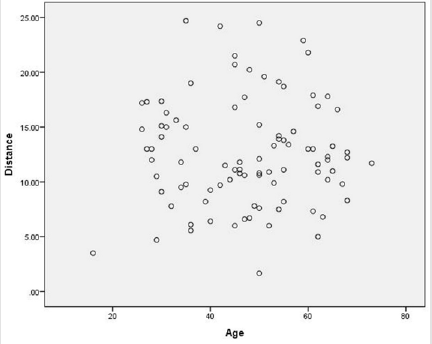
Figure 2: Scatter plot shows age in relation to the distance between TSSJ and the asterion on 3D CT bone images. The vertical axis is a line connecting the asterion and margin of TSSJ and the lateral axis is age.
Of all 94 patients diagnosed as VS preoperatively, 38 were male while 56 were female. The mean age of male patients was 46.26 ± 14.60 years while the mean age of female patients was 47.96 ± 11.84 years, which is of no statistical significance (P=0.536), which assists in excluding the influence of age on the distance between TSSJ and the asterion (occipitomastoid suture) when the comparison is between genders (Figure 2). In male patients, the distance from TSSJ to the asterion was 12.55 ± 5.26 mm while in female patients, the distance was 12.82 ± 4.68 mm. The difference of the distance between male and female is not statistically significant (P=0.794), which illustrates that the distance between TSSJ and occipitomastoid suture may not be associated with genders (Figure 3). Among patients, 44 were found with the tumor on the left side while 50 on the right side. Surprisingly, we found a significant difference between left side and right side for the distance from TSSJ to the asterion (P=0.006) (Figure 4). For left sides, TSSJ was anterior to occipitomastoid suture at a distance of 11.24 ± 5.14 mm. For right sides, TSSJ was anterior to the asterion at a distance of 14.00 ± 4.32 mm. In our samples, the location of TSSJ was all anterior to the asterion, and the distance was 12.71 ± 4.90 mm (Figure 5). A scatter plot was used to evaluate whether there is linear correlation between the distance and age, and the correlation coefficient was -0.003, which strongly indicates that the distance between TSSJ and occipitomastoid suture is not associated with age (Figure 2).
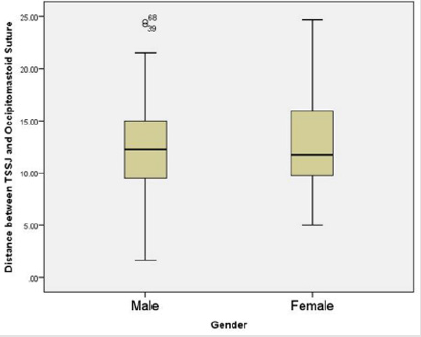
Figure 3: The box diagram illustrates that the distance between TSSJ and occipitomastoid suture does not statistically difference between male and female.
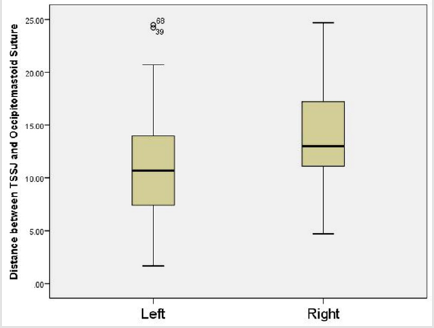
Figure 4: The box diagram illustrates that a significant difference exists between left side and right side in the distance from TSSJ to the occipitomastoid suture.
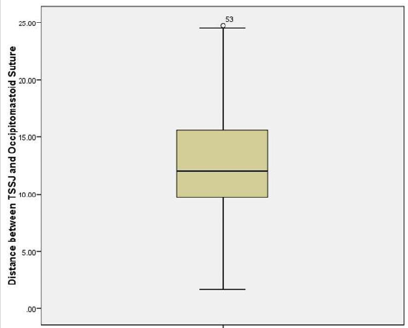
Figure 5: The box diagram displays the distance between TSSJ and occipitomastoid suture in our series.
Discussion
The retrosigmoid craniotomy is usually performed to gain access to the CPA. Traditional superficial landmarks affected the accuracy of the venous sinuses location, particularly with regards to where this relationship may result in unsafe and/or complicated surgical access [4-6]. In such procedures, accurate localization of the sigmoid sinus, and the transverse and sigmoid sinuses junction (TSSJ) is imperative to reduce the risk of the venous sinus injury. An accurate localization of the real position of the TSSJ was available in this series through preoperative imageguided individualized anatomical localization method. The method combining preoperative image with intraoperative skull anatomical landmarks is accurate and practical for identifying the TSSJ and establishing the relationship between the location of the asterion and the TSSJ during retrosigmoid craniotomy. How to identify the correct burr hole placement for retrosigmoid craniotomy has been widely explored in order to avoid sinuses injury and precisely expose the inferior edge of the transverse (superiorly) and the posterior margin of the sigmoid sinuses (inferiorly) [7-9].
A burr hole medial to the TSSJ can reveal the margin of the TSSJ with the least risk. In the present study, we found the asterion lie directly over the inferior margin of the transverse sinus in 97.87% of cases, so the distance from the intersection of the asterion and occipitomastoid suture to the TSSJ is the shortest between the occipitomastoid suture and the sigmoid sinus. The posterior border of the mastoid process can be used as a parameter to identify the posterior margin of the sigmoid sinus [10]. Illumination of mastoid air cells correlates well with the sigmoid sinus in the retrosigmoid approach [11]. In clinical practise, we found these methods do not reflect the exact position of sigmoid sinus, and mastoid air cells vary largely in different patient.
Although neuronavigation can achieve an accurate definition of the target area, it brought out more damage to patients because of installing Mayfield clamps and add preoperative and intraoperative procedures [11]. Briefly speaking, neuronavigation is invasive and produces extra time and costs. Some authors described a high incidence of venous injury based on image-guided retrosigmoid craniotomy, different with ours [2,3].
In our series, the sigmoid sinus burst did not occur. In the present study, the umbriferous position of TSSJ, indirectly located by the preoperative image, can confirm the burr hole placement during surgery. Every patient has distinctive location relationship between the asterion (occipitomastoid suture) and the TSSJ. Previously we have illustrated that the distance between TSSJ and occipitomastoid suture is not associated with age or gender, which pushes our work into a more universal level and easier to apply to most patients. CT scan imaging, especially bone window, is superior to MRI to study bone features, but the T1WI MRI sequence was clearer in indicating the transverse and sigmoid sinuses, which was helpful for determining the distance from the intersection of the asterion and occipitomastoid suture to the TSSJ [9,10]. In our series, the distance on the base of CT scan images combined with MRI images can be obtained. In the operation, the venous sinuses and anatomical landmarks can be drawn in the bone surface. In retrosigmoid craniotomy, neurosurgeons usually depend on surface landmarks on bone and their experience to evaluate the position of venous sinuses and estimate an appropriately initial burr-hole, which is not accurate each time because of variability in different patients.
In the previous study, many neurosurgeons have established their own method to locate sigmoid sinus. The author measured the x and y coordinates of the anterosuperior point of transverse‑sigmoid sinus junction and the squamosal‑parietomastoid suture junction to define a rectangular coordinate system [11]. However, the measurement is based on skull samples instead of patients alive, where there might be some measurement bias. The sample size was also too small to generalize this method in clinical application. The author locates the TSSJ based on 3D-CT in retrosigmoid craniotomy, but not all hospitals are equipped with 3D-CT images and its accuracy is not high [12]. In our present study, we introduce a simplified procedure based on MRI and CT to localize the TSSJ in retrosigmoid craniotomy, and the location of sigmoid sinus. 94 patients who underwent retrosigmoid craniotomy were analyzed. On the internal view of skull in MRI, we measured the distance between TSSJ and the intersection of the asterion and occipitomastoid suture of every patient. Such distance is reflected as red line labeled on the outer surface of cranium indicated in Figure 2.
This simple method could help in localizing the sigmoid sinus and TSSJ and avoiding the risk of sinus injury and reducing the bone defect. The method do not need to establish any coordinate system, so it is convenient but sufficiently precise for practical application at surgical planning. Because surface landmark in the literature for identifying the transverse TSSJ junction is unreliable, we have attempted to refine this location method with the largest sample size to date. These data can assist surgeons to localize the preoperative projection and intraoperative location of the TSSJ when surface landmark are not accurate. We studied relations of the external landmarks with the venous sinuses, of which the anatomic position was variable. Knowing the location of the venous sinuses avoid inadvertent entry into the venous sinuses and limitation of the size of the bony opening.
Interestingly, we found a significant difference between left sides and right sides for the distance from occipitomastoid suture to TSSJ (P=0.006) in our series. The distance on the right side is longer than that on the left side at a distance of 2.76 mm on average.
This might be due to different size of transverse sinuses in between left sides or right sides. Hwang RS et al. found that the right and left TS were constantly different in size and the right TS was more often larger than the left TS [13]. This may guide neurosurgeons to pay attention to such a difference during craniotomy since the tumor is on different sides. Ribas et al. performed measurements on 50 sinuses from 25 dried skulls [6]. He found that TSSJ occurred approximately 1 cm in front of the asterion, which is in accordance with our result. Anatomical landmarks complemented with preoperative images offer a simple and reliable method in the identification of the TSSJ position for retrosigmoid craniotomy. This method significantly promotes speed and safety in the retrosigmoid approach and decreases venous sinus injuries, which displayed the reliability of our study in the location of TSSJ in all cases of our series.
Conclusion
Anatomical landmarks combined with preoperative image location as described in this paper is an easy, fast and safe method for the localization of TSSJ for retrosigmoid approaches, which closely matches the individual anatomy of the patient and reduces the risk at injury to the hidden venous sinuses. In the retrosigmoid approach, the advantage of localizing the projection of the TSSJ beyond bone barrier before actually dissecting them provides additional precision and safety for the patient by ready and accurate localization of the transverse-sigmoid sinus complex.
Limitation
One of the limitations of our study was that we only measured the distance from TSSJ to the occipitomastoid suture in the asterion plane. It is reported that in some cases the TSSJ was below the asterion plane, which is uncommon. Another limitation was that most of our patients were adults, which limits our result applicating to adults only. In the future, the distance from TSSJ to occipitomastoid suture remains measuring. In conclusion, the method combining preoperative image and intraoperative anatomical landmarks discards complicated coordinate system and provides a convenient way for neurosurgeons to locate the TSSJ more practically and precisely.
Acknowledgement
Not applicable.
Author contributions
All authors contributed equally to the paper. WCW, XRN, XYG and ZYL drafted the manuscript. XLW, ZL and YZ performed data collection. HBL, JML and JZ supervised the data collection and revised this article. All authors read and approved the final manuscript.
Funding
This study was supported by the Fundamental Research Funds for the Central Universities (grant number 19ykpy190).
Availability of Data and Materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The study accorded to the ethical guidelines of the Declaration of Helsinki. Written informed consent was obtained from all these patients. All authors have approved the final article.
Consent for Publication
Not applicable.
Competing Interests
The authors declare that there is no conflict of interests.
References
- Da Silva EB, Leal AG, Milano JB, Da Silva LF, Clemente RS, et al. (2010) Image-guided surgical planning using anatomical landmarks in the retrosigmoid approach. Acta Neurochir (Wien) 152(5): 905-910.
- Gharabaghi A, Rosahl SK, Feigl GC, Safavi Abbasi S, Mirzayan JM, et al. (2008) Image-guided lateral suboccipital approach: part 2-impact on complication rates and operation times. Neurosurgery 62(3Suppl 1): 24-29.
- Hamasaki T, Morioka M, Nakamura H, Yano S, Hirai T, et al. (2009) A 3-dimensional computed tomographic procedure for planning retrosigmoid craniotomy. Neurosurgery 64(Supply 5): 241-245.
- Day JD, Fukushima T, Giannotta SL (1996) Innovations in surgical approach: lateral cranial base approaches. Clin Neurosurg 43: 72-90.
- Lang J, Samii A (1991) Retrosigmoid approach to the posterior cranial fossa: an anatomical study. Acta Neurochir (Wien) 111(3-4): 147-153.
- Ribas GC, Rhoton AL, Cruz OR, Peace D (2005) Suboccipital burr holes and craniectomies. Neurosurgical Focus 19(2): E1.
- Tanaka Y, Kobayashi S, Unoki T, Nagashima H, Iwashita T (1995) Illumination of Mastoid Air Cell for Suboccipital Craniotomy. Neurosurgery 36(5): 1049-1051.
- Roberts DW, Strohbehn JW, Hatch JF, Murray W, Kettenberger H (1986) A frameless stereotaxic integration of computerized tomographic imaging and the operating microscope. Journal of Neurosurgery 65(4): 545-549.
- Hill DL, Hawkes DJ, Crossman JE, Gleeson MJ, Cox TC, et al. (1991) Registration of MR and CT images for skull base surgery using point-like anatomical features. The British Journal of Radiology 64(767): 1030-1035.
- Pérez AJ, Hernández LC, Ornia M, García Y (2006) The noninvasive study of cerebral veins and dural sinuses: comparison of two MR angiography technique. Radiología 48(2): 87-98.
- Li RC, Liu JF, Li K, Qi L, Yan SY, et al. (2016) Localization of Anterosuperior Point of Transverse-sigmoid Sinus Junction Using a Reference Coordinate System on Lateral Skull Surface. Chin Med J (Engl) 129(15): 1845-1849.
- Xia L, Zhang M, Qu Y, Ren M, Wang H, et al. (2012) Localization of transverse-sigmoid sinus junction using preoperative 3D computed tomography: application in retrosigmoid craniotomy. Neurosurg Rev 35(4): 593-598.
- Hwang R, Turner R, Radwan W, Singh R, Lucke Wold B, et al. (2017) Relationship of the sinus anatomy to surface landmarks is a function of the sinus size difference between the right and left side: Anatomical study based on CT angiography. Surgical Neurology International 8(1): 58.
