 Research Article
Research ArticleAbstract
The present study was to identify some responsible variables for the prevalence of diabetic retinopathy among adult people of Bangladesh. To fulfil the objective of the study, statistical analysis was done utilizing the data collected from 960 adults of both urban and rural areas of the country. The data were collected by some doctors and nurses from and nearby their working places. Among the investigated adults, 15.8 percent were suffering simultaneously from diabetes and retinopathy and majority (40.8%) of them were suffering for five to less than 10 years. More prevalence of the disease was observed among females, married persons, adults of ages 40 years and above, physically inactive group of persons, adults engaged in sedentary activities, higher income group of adults, obese group of people, adults of hypertension and among those who were taking can foods . The most responsible identified variables were age followed by family income and expenditure, marital status, utilization of time and duration of disease. These variables were identified by factor analysis.
Keywords: Diabetic Retinopathy; Socioeconomic Variables; Odds Ratio; Risk Ratio; Confidence Interval of Odds and Risk Ratios; Factor Analysis; Factor Loadings
Introduction
Diabetes is a disease which affects the body parts like kidneys, heart, eyes, sensory system and so-forth. The eyes are affected by different diseases. One of the deadliest diseases in the eye is retinopathy and it occurs due to diabetes, blood glucose, etc. It happens when high blood sugar levels damage blood vessels in the retina. So, the disease is called diabetic retinopathy (D.R). It starts due to delayed and untreated diabetes and it is the second largest one which occurs among the human beings [1,2]. The disease is the leading cause of blindness and visual impairment affecting 30 – 40 percent of diabetic patients of age 40 years and above [3-6]. The number of people with blindness due to DR and low vision were estimated 400000 and 2.6 million, respectively, both almost double since 1990. The projections for diabetic complications for 2020 are in increasing trend. For Southeast Asia the projected numbers are 30000 and 216ooo, respectively [7,8]. The risk of visual impairment due to diabetes was increased generally by 2.6 times for people below the age of 60 years and 12.0 times for those over 60 years. There were well described risk factors for the development of DR. The most and clearly recognized factors are duration of diabetes, the degree of glycaemic control measured as glycosylated haemoglobin. In addition to that, hypertension, dyslipidaemia, smoking, age, Body Mass Index (BMI), were also identified as risk factors of diabetic retinopathy [3,8-14]. Besides these factors some biological factors were also identified as the risk factors of DR [15-25]. In the present paper, attempts were made to identify the responsible socioeconomic variables for the incidence of diabetic retinopathy among adult people of Bangladesh.
Methodology
The source of the analytical results presented in this paper was the data collected from 960 adults of ages 18 years and above residing in Both urban and rural areas of Bangladesh. The data were collected by some doctors and nurses when they were completing their Master of Public Health degree in American International University – Bangladesh during the session 2017–18. The adults were investigated by quota sampling method, where the targeted adults were 1000 to cover around 700 diabetic patients as 70 percent diabetic adults were observed in a separate study [26]. It was also decided to investigate the remaining 300 adults as control group. The plan of investigation of 700 diabetic patients was made to ensure a good number of diabetic retinopathy patients. But during investigation 672 diabetic and 288 normal subjects were interviewed due to some constraints in doing the survey. Finally, the data were recorded from 960 adults. The data were recorded through a pre-designed and pre-tested questionnaire. The questionnaire contained questions related to different socioeconomic variables including the family income and expenditure of each of the adults. From diabetic patients, the information on duration of disease, complications facing due to the disease, level of blood pressure, etc, were also recorded. From all sample units, data on utilization of time, physical labor, food habit, etc. were also noted.
Some of the variables were qualitative in nature and some were quantitative in character. For analytical purpose, all the variables were transformed to nominal scores by assigning numbers. The association of diabetic retinopathy with different social and economic variables were investigated by Chi-square test. The association of DR with Body Mass Index (BMI) was also investigated. BMI was measured by weight (in kg) divided by height (in metre2). The respondents were classified as underweight [ BMI < 20], normal [ 20 < BMI < 25], overweight [ 25 < BMI < 30]and obese [ BMI ≥ 30]. The significant association was decided when the p-value of any Chi-square test was less than or equal to 0.05. To decide the risk of DR for adults the risk ratio was calculated along with its 95% confidence interval considering the prevalence of the disease for a level of any socioeconomic variable [27-32]. To identify the responsible variable for diabetic retinopathy, factor analysis was done for eigen value 2 so that maximum variation in the data set of diabetic retinopathy patients was explained. The analysis was done using SPSS version 25.
Result
The total investigated adults were 960. Out of them, the number of diabetic adults was 672 and 152 of them were suffering from diabetic retinopathy. The analytical results were prepared by classifying the adults in two groups, in one group there were 152 patients of DR and in another group, there were 808 adults including 288 normal subjects. Among the DR patients, 40.8 percent were suffering from the disease for 5 years to less than 10 years. The percentages of patients suffering for less than 5 years, 10 years to less than 15 years and 15 years and above were 18.4, 21.1 and 19., respectively. The percentage of rural adults was 43.5 and 16.5 percent of them were patients of DR. The corresponding percentage among urban adults was 15.3. The prevalence of DR among urban and rural adults was almost similar [χ2 = 0.252 p-value = 0.615] (Table 1). The risk ratio [ R.R. = 1.04; confidence interval, C.I. (0.77, 1.42)] also indicated that both urban and rural adults were at similar risk of the disease. Both groups were similarly exposed to the disease [ O.R. = 1.09; C.I. (0.77,1.54)]. Among the investigated units’ 55.2 percent were males and 10.2 percent of them were DR patients.
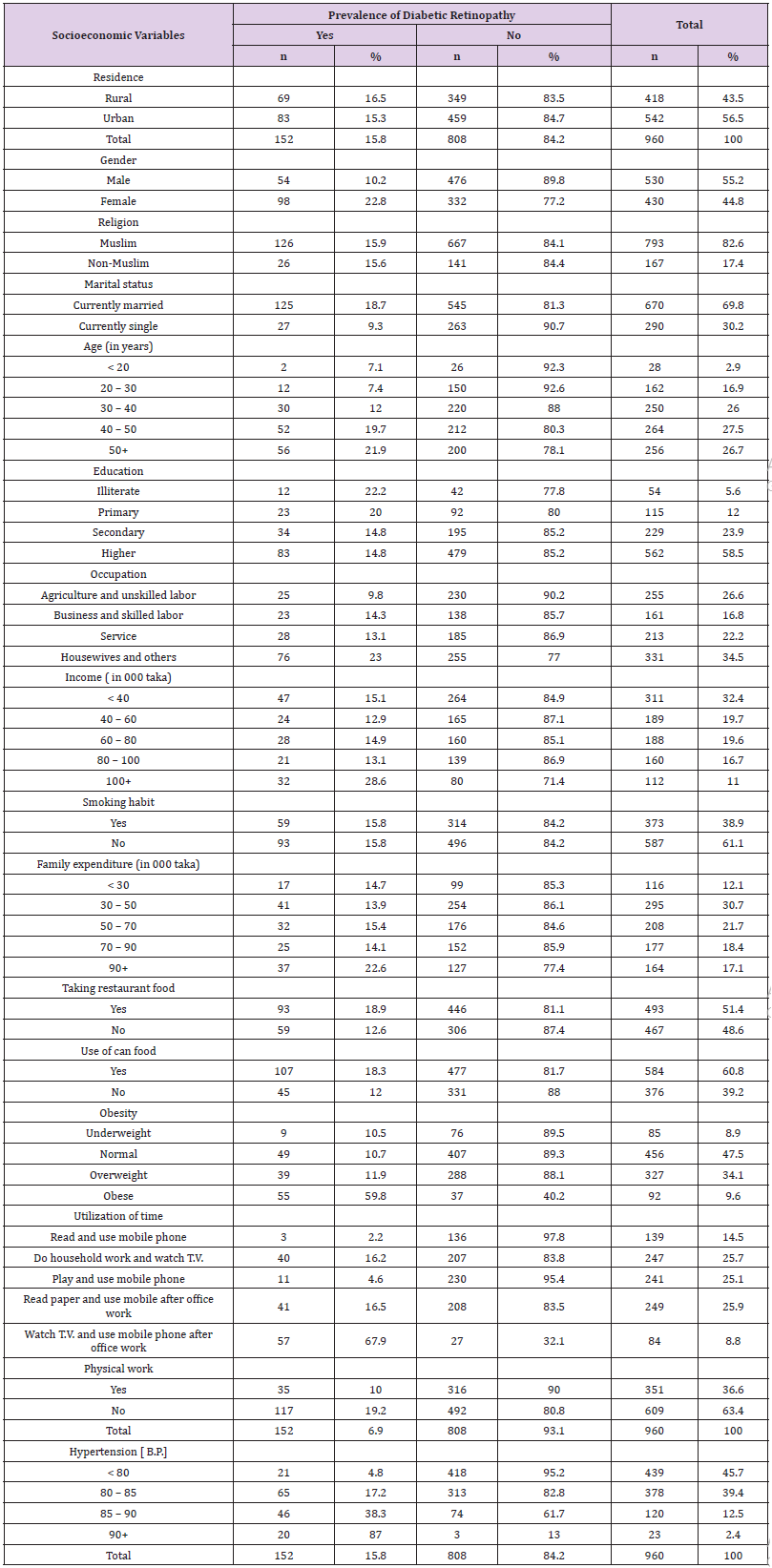
Table 1: Distribution of adults according to socioeconomic variables and prevalence of diabetic Retinopathy.
There was significant difference in the rates of DR patients of males and females [χ2 =28.291, p- value = 0.000]. The females were more than two times exposed to the disease than the males [ O.R.= 2.60; C.I. (1.81,3.3)]. For them the risk of the disease was also more than two times than the risk of males [ R.R.= 2.24; C.I. (1.6, 3.01)]. The percentage of Muslim respondents was 82.6 and 15.9 percent of them were DR patients. Among the non-Muslim respondents’ 15.6 percent were also DR patients. However, there was no significant differences in the proportions of DR patients among the Muslim and non-Muslim respondents [χ2 =0.011, p-value=0.918]. Both the religious groups were similarly exposed to the disease [O.R.= 1.02; C.I. (0.64, 1.62). R.R.= 1.02; C.I. (0.47 ,2.21)]. From the study, it was noted that age and diabetic retinopathy was significantly associated [χ2 = 22.943, p- value = 0.000].
The proportion of DR patients among adults of ages 40 years and above (53.2%) was 0.262. This proportion was too high compared to the overall proportion of DR patients in the sample. They were more than 4 times exposed to the disease compared to that of adults of ages below 40 years [ O.R.=4.07; C.I. (2.79, 5.94)]. The relative risk of the disease for them was 3.26 [ R.R.=3.26; C.I. (2.41, 4.37)]. Among the adults, 69.8 percent were currently married, and 15.9 percent of these married group were affected by the disease. The percentage of currently unmarried adults suffering from the disease was 9.3. Marital status was significantly associated with the prevalence of diabetic retinopathy [χ2 =13.267, p-value = 0.000]. The married adults were more than two times exposed to the disease compared to that of unmarried adults [ O.R.= 2.23; C.I. (1.26, 3.95)]. The married persons had two times risk of the disease compared to the risk of single adults [ R.R.= 2.00; C.I.( 1.0,3.3 )].Level of education and prevalence of diabetic retinopathy was not associated for this group of adults as was observed by Chi-square test [χ2 = 3.797, p-value= 0.284. However, more illiterate and primary educated adults (20.7%) were affected by the disease and this group was one and half time more exposed to the disease compared to that of secondary and higher educated adults [O.R.= 1.50; C.I.(0.98, 2.28)]. Their risk for the disease was 40 percent more than the risk of other educated adults [ R.R.= 1.40; C.I. (0.72, 2.72)].
The investigated adults were classified into four groups according to their occupation. These groups were farmers and unskilled labors (26.6%), businesspersons and skilled workers (16.8%), service persons (22.2%) and housewives and students (34.5%). The first group rendered physical labor. The other three groups were not directly involved in physical labor. The grouping was done to observe the risk of DR for the adults who were physically inactive, because physical inactivity was identified as the responsible factor for diabetes [ 26,29]. The proportions of DR affected adults of different occupational patterns were significantly different [χ2 =21.018, p-value = 0.000]. The biggest group (34.5%) of adults were housewives and students and higher proportion (23.0%) of them were the patients of DR. This proportion was too high compared to the overall proportion (15.8%) of DR patients in the sample. They were more than two times exposed to the disease compared to that of other adults [ O.R.= 2.17; C.I. (1.53,3.08)]. They were at higher risk of the disease by 90 percent [R.R.=1.90; C.I. (1.28, 2.82)]. The investigated adults were classified into five classes according to their family income. The adults having highest income (Taka 100 thousand and above) were 11.7 percent and 28.6 percent of them were affected by the disease. This percentage of affected group was too high compared to the overall affected respondents in the sample. The proportions of affected adults of other income levels were similar to the overall affected adults in the sample. However, proportions of affected adults of different family income levels were significantly different [χ2 = 16.157, p-value = 0.003]. This significant difference was noted mainly for the adults of higher income group. This group was more than two times exposed to the disease compared to other groups of adults [ O.R.= 2.43; C.I. (1.54,3.52]. The relative risk for them was also more than two times [ R.R.=2.02; C.I. (1.48,3.01)]. Level of family expenditure was not associated with the Prevalence of DR [χ 2 =6.939, p-value = 0.139]. But the adults (17.1%) of families spending highest amount of money (Taka 90 thousand and above) were affected more (22.6%) by the disease. This proportion was too high compared to that of other adults. The relative risk was also more than 5 times compared to the risk of other adults above [ O.R.= 11.82, C.I. (7.41, 18.86); R.R.= 5.35, C.I. (2.49, 11.51)]. To the proportion of overall affected respondents in the sample. This group of adults were 73 percent more exposed to the disease compared to the adults belonging to the families spending less than Taka 90 thousand. The relative risk of the disease for this group of adults was also higher [ O.R. = 1.73, C.I. (1.14, 2.62; R.R.= 1.56, C.I. (0.81, 3.02]. Significant association was observed between food habit of the adults and prevalence of diabetic retinopathy [χ 2 = 6.985, p- value= 0.008]. Majority (51.4%) of the respondents were habituated in taking food from restaurant and 18.9 percent of them were suffering from DR. This group of adults were 61 percent more exposed to the disease compared to that of adults who did not take restaurant food [ O.R. = 1.61, C.I. (1.13, 2.29]. The relative risk of the disease for this group of adults was also higher compared to the risk for adults who did not take restaurant food [R. R= 1.49, C.I. (0.68, 3.26]. Significant association between habit of taking can food and prevalence of diabetic retinopathy was observed [ χ2 = 6.93, p-value =0.00]. Among the adult’s 60.8 percent were habituated in taking can food and 18.3 percent of them were affected by the disease. This affected group was 65 percent more exposed to DR [ O.R.= 1.65, C.I. (1.13, 2.85]. The relative risk of the disease for this group was also high [R.R.= 1.53, C.I (1.0, 2.19)]. Obesity and prevalence of diabetic retinopathy was significantly associated [χ2 =147.703, p- value =0.000]. Among the investigated adult’s 9.6 percent were obese and 59.8 percent of them were DR patients. The rate of DR affected patients was in increasing trend with the increase in level of obesity.
The obese adults were around 12 times more exposed to the respondents replied to a question regarding the utilization of time outside their normal duties. Some replied that they passed their time using mobile phone and reading ( 14.5%), some were doing the household work and watching T.V.( 25.7%), some were playing and using mobile phone ( 25.1%) , for another group the mode of passing time was paper reading and use of mobile phone ( 25.9%) and a smaller group ( 8.8%) passed their time using mobile phone and watching television. But 67.9 percent of the last group were suffering from diabetic retinopathy. They were exposed to the disease more than 17 times compared to that of other adults [ O.R.=17.36, C.I. (10.98, 28.70)]. For this group the risk of the disease was more than 6 times than the risk of the disease of other adults. Significant association was observed between utilization of time and prevalence of diabetic retinopathy [χ2 =213.167, p – value = 0.000]. Passing time only by reading paper, using mobile phone and watching television without any physical work is sedentary activity and it is the cause of many diseases [26]. In this study, a big group of adults (34.7%) were involved in sedentary activities and they were more than 5 times exposed to the disease [ O.R.= 5.48, C.I (3.77,7.97)]. Among the investigated adult’s 36.6 percent were doing some sorts of physical work. This group of adults were less affected by DR (10.0%). Those who did not do any physical work 19.2 percent of them were suffering from DR. Physical inactivity was significantly associated with the prevalence of DR [χ2 =14.266, p- value = o.000]. The physical inactive group was more than two times exposed to the disease compared to that of other group [ O.R.= 2.15, C.I. (1.44,3.22); R.R. = 1.93, C.I.(1.28, 2.92)]. Earlier it was reported that hypertension was significantly associated with D.R. [6]. To study association of hypertension and diabetic retinopathy, the record of diastolic blood pressure was utilized. It was noted that the diastolic blood pressure level of 45.7 percent adults was less than 80 (mmHg) and only 4.8 percent of them were suffering from DR. The blood pressure level of 39.4 percent adults was more than 80 but less than 85. The percentage of DR patients among this group was 17.2. The percentages were in increasing trend for adults having blood pressure level 85 and more. There was significant association between hypertension and diabetic retinopathy [χ2 =173.639, p – value= 0.000]. This letter group of adults were more than 7 times exposed to the disease. For them, the risk of the disease was also higher compared to the risk of adults who had blood pressure less than 85 [ O.R. = 7.29, C.I. (4.90, 10.85); R.R.= 4.38, C.I. (2.53, 7.59)].
Factor Analysis
The analytical results presented above indicated that except residence, religion and education all other socioeconomic and epidemiological variables were significantly associated with diabetic retinopathy. Different variables were associated in different degrees. The odds and risk ratio gave some idea regarding the responsible variables for the prevalence of diabetic retinopathy. But neither Chi-square test nor odds and risk ratio identify the most responsible factor for the DR. Factor analysis and some other statistical analyses can identify the most important variables for the variation in any characteristic under study. In the present case, factor analysis was performed using the available dependent variables for the diabetic retinopathy. The biggest factor loading of a variable after the analysis indicates the most responsible variable for the variation in the characteristic [30-32]. During the analysis one result known as communality give the initial idea about the importance of a variable to be retained in the analysis. In some cases, a value of communality 0.40 or less for a variable leads the researcher to drop that variable from the analysis. The results observed in doing the analysis of the present data were shown in Table 2 above:
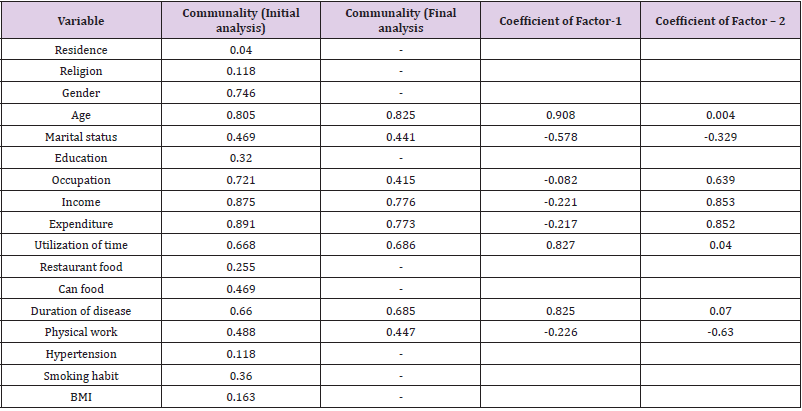
Table 2: Maternal age, education and family income.
The variables included in the analysis was satisfactory as KMO = 0.586, χ2 =1141.176, p-value = 0.000. After the initial analysis, some variables were dropped as the communalities of those variables were less than 0.40. The results of the analysis at third and final step were shown in the tables. At this stage the value of KMO= 0.584, χ2 =960.153, P- value = 0.000. This result justified the inclusion of the variables in the final analysis. The analysis provided two factors. Both the factors explained 63.107 percent variation in the data of patients of diabetic retinopathy. The first factor indicated that the most responsible variable for DR was age followed by utilization of time and duration of the disease. The second factor indicated that the responsible variable was income followed by expenditure and occupation. Physical work was also an important variable to explain the variation in the data set of patients of DR.
Discussion
The paper dealt with the analysis of data collected from 960 adults residing in both urban and rural areas of Bangladesh to study the impacts of some socioeconomic characteristics on diabetic retinopathy. Among the investigated adults, 15.8 percent were suffering from DR. Majority (40.8%) of these patients were facing the problem for 5 years to less than 10 years. Another 19.7 percent were suffering for 15 years and above. Again, 27.5 percent adults were in the age group 40 to 50 years and 19.7 percent of this group of adults were the patients of DR. The study indicated that age of adults and diabetic retinopathy was significantly associated and adults of ages 40 years and above were more than 4 times exposed to the disease. Similar findings were noted in both home and abroad [3,4,5,12]. The rural (43.5%) and urban adults were at similar risk of the disease. But females were at higher risk of the disease [ R.R. = 2.24]. The proportions of prevalence of DR for males (0.102) and females (0.228) were significantly different. Females were more affected by the disease. Similar finding was noted abroad [5]. The females were more than two times exposed to the disease [0. R.= 2.60]. But Muslim and Non-Muslim adults were at similar risk of DR. Most (69.8%) of the adults were married and 18.7 percent of them were patients of DR. Their relative risk of the disease was more than two times compared to the risk of single adults. Level of education was not significantly associated with the prevalence of diabetic retinopathy. However, illiterate and primary level educated adults together were 50 percent more exposed to the disease compared to that of secondary and higher educated adults. More illiterate adults (22.2%) were affected by the disease. Level of occupation was significantly associated with the prevalence of DR. Females and students were not directly involved in physical activity [29] and their relative risk of the disease was around two times compared to the risk of other adults. This group of respondents were higher in percentage compared to the percentage of other occupational groups. As in this group there were more females, the group was more exposed to the disease. This phenomenon was already stated in studying the association of sex and prevalence of diabetic retinopathy. It was already mentioned that females were at higher risk of diabetic retinopathy [6]. Majority (32.4%) of the adults belonged to the families of the lowest income group (Taka < 40 thousand per month). The adults of these families facing the problem of DR were lower in proportion compared to the proportion of diabetic retinopathy patients in the overall sample. Lower proportion of DR patients was also observed in the middle-income group of families (income 40 - < 60 thousand taka). But significant, association of income and prevalence of DR was observed from the analysis. The significance was noted due to the findings were reported in abroad [5,12,13]. The adults having blood pressure 85 mmHg and above were more than 7 higher (28.6%) proportion of DR patients in the families of higher income. These adults of DR patients in the highest income group of families were at risk more than two times compared to the risk of adults belonging to the families of other income levels. The adults (17.1%) belonging to the families spending highest amount of money (Taka 90 thousand and above) were suffering more in proportion. For this group of adults, the risk of the disease was 56 percent more than the risk for the adults of families spending money less that taka 90 thousand per month. However, monthly expenditure pattern and prevalence of DR were not significantly associated.
Body mass index was significantly associated with the prevalence of diabetic retinopathy. This phenomenon was observed in both home and abroad [6,13,14]. This study indicated that the risk of the disease for the obese adults was more than 5 times compared to the risk of other adults. The sedentary activities of the adults were significantly associated with the prevalence of diabetic retinopathy. Those who passed their time by reading paper and watching television (16.1%) outside their normal routine work, they were more exposed to the disease. For such group of adults, the risk of the disease was more than two times than the risk other adults. Another significant responsible factor for diabetic retinopathy was hypertension. Similar times exposed to the disease. For this group, the risk of the disease was more than 4 times than the risk of disease of other adults. Majority (51.4%) of the respondents were habituated in taking restaurant food. This food habit of the adults was significantly associated with the prevalence of diabetic retinopathy and those who were habituated in taking restaurant food were at higher risk of the diabetic retinopathy compared to the risk of adults who were not taking restaurant food. Similar was the case for them who were used to take can food. Further, physically inactive adults were also at higher risk [RR. = 1.93] of the disease and a big group (63.4%) was physically inactive. So far, the results related to the study of association of socioeconomic and some biological variables with prevalence of diabetic retinopathy was discussed. Some variables were associated with DR, but the study of association did not identify the most responsible variables for the variation in the data of DR patients. To identify the most responsible variables factor analysis was done, where highest factor loading indicated the most responsible variable for the variation in the data of patients of diabetic retinopathy. The analysis identified age as the most responsible variable for diabetic retinopathy followed by utilization of time and duration of disease. The other responsible variables were family income, family expenditure and physical inactivity.
Conclusion
The information presented in the paper were the analytical results collected from adults of 18 years and above residing in both urban and rural areas of Bangladesh. The data were collected by some doctors and nurses utilizing the technique of quota sampling. Seven hundred diabetic patients and 300 normal adults were the target units for data collection as in some previous study [25] around 70 percent diabetic adults were found out. Among the current investigated 960 adults, 67.9 percent were diabetic patients and 32.1 percent were normal subjects. Among the diabetic patients, 23.3 percent were suffering from DR. The percentage of DR patients in the overall sample was 15.8. Binary classification was done to observe the association and risk ratio and odds ratio for exposed DR patients compared to non-DR adults. One component of binary classification was the adults of two groups and another component was socioeconomic and biological variable. This latter component includes residence, religion, gender, age, marital status, education, occupation, income, expenditure, food habit, physical activity, utilization of time, blood pressure, and body mass index.
In the sample, 43.5 % were rural residents, 55.2% were males, 82.6% were Muslim adults, 69.8% were currently married adults, 54.2% were of the ages 40 years and above, illiterate and primary educated adults were 17.6%, housewives and other occupational groups were 34.5%, percentages of rich families in terms of income and expenditure were 11.7 and 17.1 respectively. Percentages of obese, physically inactive adults and adults having blood pressure 85 mmHg and above were 14.5, 63.4 and 14.9, respectively. The percentages of adults habituated in taking restaurant food and can food were 51.4 and 60.8 respectively; 8.8 percent adults were involved in sedentary activities. Among the diabetic retinopathy patients 18.4 % were suffering for less than 5 years, 40.8% were suffering for 5 years and above but less than 10 years, 21.1% were suffering for 10 years and above but less than 15 years and the remaining 19.7% were suffering for 15 years and above. The analysis showed that the risk of diabetic retinopathy was higher for females, married adults, adults of ages 40 years and above, illiterate and primary educated adults, housewives and other occupational group of adults, adults of rich families in terms of income and expenditure, adults involved in sedentary activities, physically inactive adults, adults habituated in taking restaurant and can food and adults those who were in hypertension.
The analysis of association of DR with some socioeconomic and biological variables were done. Irrespective of significant or insignificant association, the degree of the risk of the disease due to some socioeconomic variables was evaluated. But this measurement of the risk ratio or odds ratio did not indicate the most responsible variable for the disease. The responsible variable was identified by factor analysis. The most responsible variable for the disease was age followed by utilization of time by the adults and the duration of the disease. The other responsible variables for the disease were family income and family expenditure followed by physical inactivity. From the analytical results it could be said that some of the social factors would be responsible for obesity, diabetes and diabetic related diseases. So, it cannot be avoided but there should be some attempts to reduce the intensity of obesity, diabetes and hence diabetic related diseases. For this, people should be motivated to avoid the sedentary activities so that they themselves can manage better and healthy life throughout their life span. The following aspects can be considered, and attempts should be made to follow some norms which are essentials for better health management.
a. There should be some campaign to explain the need of avoiding the prevalence of non-communicable diseases by the health management authority and people should be advised to join the campaign in which the health hazard can be detected and accordingly they should be advised to consult the health workers for the treatment,
b. People should be advised to take such foods which do not create the problem of obesity and obesity-oriented diseases,
c. People should avoid restaurant food, can food and foods of high calorie, salts and saturated fats,
d. People should be advised to avoid sedentary activities like watching television, using mobile phone and smart phone as per as possible,
e. People should be suggested to do some physical labor as and when they get the chance, or at least they can develop a habit of morning or evening walk,
f. Health authority in urban and rural area can provide a free service to the people at least in a month to check up their blood pressure, blood sugar and body weight free of cost. This can be done by forming club, charitable trust and social workers groups.
References
- (1997) World Health Organization, Global initiative for the elimination of avoidable blindness. An informal consultation.
- (2006) World Health Organization, Consultation of Diabetes Mellitus.
- Lee VS, Kingsley ET (1993) The diagnosis of diabetic retinopathy, Opthalmoscopy vs fundus photography, Jour Opthalomogy 100: 1504-1512.
- (2017) World Health Organization, Nepal Tackles Diabetic Retinopathy, WHO Report.
- (2019) World Health Organization, Monitoring Health for SDGs. WHO.
- Maya GP (2019) Diabetic retinopathy and blindness an epidemiological overview, Intech Open.
- Omar S, Amelia G, Nancy S, Sara B, Merely G (2018) Implementation of a diabetic retinopathy referred network. Peru, Bulletin of WHO.
- Ahmed KR, Karim MN, Bhomik B, Habib SH, Bukht MS, et al. (2012) Incidence of diabetic retinopathy in Bangladesh a 15-year follow-up study. J Diabete 4(4): 386-391.
- Mc Comish B, Charlesworth J (2018) Progress and challenges in genome-wide studies to understand the genetics of diabetic retinopathy. Annals of Eye Science 3: 46.
- Friedman DS, Ali F, Kourgialis N (2011) Diabetic retinopathy in the developing world How to approach identifying and treating underserved populations. Amer Jour Opthalmol 151(2): 192-194.
- Billah M, Rahim MA (2016) Pattern and risk of diabetic retinopathy among type-2 diabetic patients experience in a tertiary care hospital. Jou Medicine 17: 17-20.
- Akhter A, Fatema K, Ahmed SF, Afroz A, Ali L, et al. (2013) Prevalence and associated risk factors of retinopathy in a rural Bangladesh population with and without diabetes. Opthalmic Epidemiol 20(4): 220-227.
- Afroza A (2009) Diabetes Mellitus and Retinopathy in Rural Bangladesh A Population Based Study. M Phil Thesis university of Oslo.
- Klein R, Klein BE, Moss SE (1994) Relationship of hyperglycaemia to the long-term incidence and progression of diabetic retinopathy. Arch Intern Med 154(194): 169-178.
- Srinivasan S, Dehghani C, Pritchard N, Russell AW, Malik RA, et al. (2018) Opthalmic and clinical factors that predict four-year development and worsening of diabetic retinopathy in type – diabetes. Jour Diabetes Complications 32(1): 67-74.
- Hietala K, Forsblom C, Summanen P (2008) Heritability of proliferative diabetic retinopathy. Diabetes 5: 2176-2180.
- Lesli RD, Pyke DA (1982) Diabetic retinopathy n identical twins. Diabetes 31: 19-21.
- Rema M, Saravanan G, Deepa R (2002) Familial clustering of diabetic retinopathy in South Indian type-2 diabetic patients. Diabetic Med 19(11): 910-916.
- Cheung CY, Hui EY, Lee CH (2016) Impact of genetic loci identified in genome- wide association studies on diabetic retinopathy in Chinese patients of type-2 diabetes. Diabetes Invest Opthalmol Vis Sci 57(13): 5518-5524.
- Kempen JH, O Colmain BJ, Leske MC (2004) The prevalence of diabetic retinopathy among adults in the United States, Arch Opthalmol 122: 552-563.
- Tan SS, Gan A, Sabanayagan C (2018) Ethnic differences in the prevalence and risk factors of diabetic retinopathy The Singapore Epidemiology of Eye Diseases Study. Opthalmology 125: 529-536.
- Huang YC, Li JM, Lin HJ (2011) Genome-wide association study of diabetic retinopathy in a Taiwanese population. Opthalmology 118(1): 642-648.
- Ma RC (2016) Genetics of cardiovascular and renal complications in diabetes. Jour. Diabetes Investig 16(6): 139-154.
- Viswanath K (2003) Diabetic retinopathy Clinical findings and management. Community Eye Health 16(46): 21-24.
- Klein R, Klein BER, Moss SE, Davies, De Mets DL (1984) The Wisconsin epidemiological study of diabetic retinopathy ii. Prevalence and risk of diabetic retinopathy when ageat diagnosis is less than 30 years. Arch Opthalmol 102: 520-526.
- Bhuyan KC, Fardus J (2019) Level of obesity and socioeconomic factors of a group of adult people of Bangladesh A factor analysis approach. Amer, Jour. Data Mining and Knowledge Discovery 4(1): 8-14.
- Paymane A, Miranda P (2018) Images of measurements of obesity.
- Sistron CL, Garvan CW (2004) Proportions, odds and risk. Radilogy 230(1): 12-19.
- Syed MS, Debra N, Muhammad HR, Musa R, Gul N (2004) Assessing obesity and overweight in a high mountain Pakistani population. Tropical Medicine and International Health 9(4): 526-532.
- Bhuyan KC (2019) A note on factor analysis applied in medical research, Archives in Biomed Eng. And Biotech 1(4): 1-3.
- Bhuyan KC (2004) Multivariate Analysis and its Applications. New Central Book Agency(P) ltd. India.
- Yotoka T (1983) Some criteria for variable selection in factor analysis. Behaviormetrika 13: 31-45.
