 Research Article
Research ArticleAbstract
Introduction: The prevalence of dental caries and gingival problems in early childhood is high and measures for prevention and oral health promotion can contribute to improve this scenario through the adoption of adequate oral hygiene habits. The use of fluoridated toothpaste, water fluoridation, diet control, and access to dental care are also important factors for promoting oral health and quality of life in children.
Objectives: To analyze the oral hygiene habits of children aged 6 to 36 years-old from Salvador, Bahia, Brazil, in 2018.
Material and Methods: Cross-sectional study involving 632 children aged 6 to 36 months from Salvador, Bahia. Data on oral hygiene habits were collected by oral examination and application of a validated questionnaire by interview of household members.
Results and Discussion: Among the participants, 72.5% received instructions about infant oral care, which were provided by the doctor/nurse in 64.8% and by the dentist in 41.9%. Caring for the child’s teeth was considered important by 99.1% of the participants and 99.7% reported to perform oral hygiene frequently (75.8% by the parents/caregivers). Only 34.8% of the children used fluoride toothpaste and 17% shared their toothbrush. The socioeconomic conditions and education level of the mother can influence the adoption of adequate hygiene habits.
Conclusion: The children of the municipality had poor oral hygiene. Expanding access to oral health services and investment in health education actions are essential for raising the awareness of parents/caregivers in order to improve oral hygiene habits and to prevent oral diseases in early childhood.
Keywords: Early Childhood Caries; Oral Health; Oral Hygiene; Risk Factors; Pediatric Dentistry
Abbreviations: WHO: World Health Organization; SD: Standard Deviation; AAPD: American Academy of Pediatric Dentistry; UFBA: Federal University of Bahia
Introduction
The World Health Organization (WHO) defined health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” [1] .Within this context, oral health can interfere with different aspects of life, including selfesteem, social interaction and school or work performance, among others [2]. Healthy life habits are already acquired in early childhood and are generally transmitted by relatives, especially by the mother. Oral hygiene practices are considered essential for the maintenance of oral health. The earlier the child acquires these healthy hygiene habits, the greater the chance of healthy growth [3]. In Brazil, disease prevention and health promotion are encouraged by the principles of the Brazilian Public Health System (SUS) guidelines, especially in the primary care setting, through the Family Health Strategy (ESF in the Portuguese acronym). Comprehensive care includes health education as a potential measure to prevent oral diseases. Dental caries and periodontal disease are the most prevalent diseases of the oral cavity and represent a public health problem because of their high prevalence, as demonstrated by epidemiological studies conducted in Brazil [4].
Early childhood caries is a term used to describe the presence of decayed, missing or filled teeth in the primary dentition of children aged 71 months or younger. This condition is the result of the interaction of a variety of etiological factors, including dietrelated factors such as high sugar intake, incorrect or absent oral hygiene, lack of fluoride exposure, socioeconomic factors, factors related to cariogenic microorganisms, and social vulnerability [5- 9].The consequences of this disease, if untreated, are pain, edema, loss of primary teeth at an early age, delayed physical development and malocclusion, among others, which can cause problems in phonetics, mastication, and esthetics, with a serious impact on the health and growth of children. Furthermore, these conditions can reduce the quality of life of children and their caregivers [10]. Caries can be effectively prevented and controlled, substantially improving the quality of life of the child [11]. The oral health status of children is frequently associated with social factors such as household income and the caregiver’s education level, especially the mother’s [12].
According to the WHO, health education refers to “any combinations of information and education activities that enable people to know how to achieve health and to seek help when they need it”. Health education has four main goals: to keep people well informed about health care and disease prevention; to adopt health as a core value; to promote appropriate health behaviors, and to change inadequate habits or behaviors [10]. Studies have shown that educational intervention can modify hygiene habits and promote oral health [13]. Within this context, preventive measures of early childhood caries should start by raising the awareness of the child’s parents/caregivers and are fundamental for prevention of this disease. The early establishment of oral hygiene routines and adequate healthy eating habits, associated with the restricted consumption of foods with cariogenic potential, are important measures for preventing early childhood caries [14,15]. A good diet in the first year of life does not only contribute to quality of life at that age, especially oral health, but also stimulates healthy eating patterns at older ages since habits acquired during this early phase are more resistant to change. [16].
The fluoridation of tap water is the most effective and efficient approach to the collective prevention of dental caries, biofilm and incipient caries lesions, as fluoride is provided continuously at low doses [17,18]. However, prevention must comprise other individual measures such as thorough oral hygiene, diet control, and sealing of grooves. It is suggested that parents start brushing their child’s teeth at least twice a day with a child-size soft toothbrush and fluoride toothpaste as soon as the first tooth erupts. In the case of edentulous children, although controversy exists as to whether or not oral hygiene is necessary, the recommendation is that parents/ caregivers clean the oral cavity after breastfeeding with a rubber finger brush or gauze soaked in water [14,19] Regular access to oral health care in childhood is also very important since it permits the early diagnosis of oral diseases and motivates and educates caregivers regarding oral health, raising their awareness on the importance of good oral hygiene of their children [20]. The aim of this study was to evaluate the oral hygiene habits of children aged 6 to 36 months from Salvador, Bahia, in 2018.
Methods
This was a quantitative, cross-sectional study involving children aged 6 to 36 months from Family Health Units (USF in the Portuguese Acronym) in the municipality of Salvador, BA. A convenience sample was obtained, and the sample size was calculated using system data, with an estimated number of 640 children considering losses. Children aged 6 to 36 months living in areas comprising the 11 selected USF were included. A total of 632 children ranging in age from 6 to 36 months participated in the study. The data were collected by a team of 13 examiners consisting of dentists and dental students undergoing their supervised internship at the USF, who were properly selected and calibrated in the data collection, as well as oral health auxiliaries and technicians. The following data were collected by interview: household socioeconomic status, general and oral health conditions of the mother and child, and oral examination of the child, involving several variables. Variables related to the oral hygiene instructions received, sources of instruction, performing oral hygiene in the child, importance of oral health care, frequency, times, use of fluoride or non-fluoride toothpaste, the person who brushes the teeth, tooth brushing at the daycare center, and sharing the toothbrush were selected.
The response variable defined in this study was “adequate oral hygiene”, which was applied to both edentulous children and children with teeth. In the case of edentulous children, the “adequate oral hygiene” variable resulted from the sum of three variables: the person who brushes the oral cavity, considering as adequate cases in which cleaning of the oral cavity was performed by the parents/ caregivers or by the child with the help of their parents/caregivers; what was used for cleaning, considering only water as adequate; frequency, considering as adequate cases in which cleaning was performed two or more times per day. In children with teeth, the “adequate oral hygiene” variable also resulted from the sum of the three variables reported for edentulous children but with different requirements. Regarding the variable “person who brushes the child’s teeth”, tooth brushing by the parents/caregivers or by the child with the help of their parents/caregivers was considered adequate. For the second variable, the answer was only considered adequate when the participants reported the use of fluoride toothpaste. Finally, regarding frequency, tooth brushing two or more times per day was considered adequate.
The study was approved by the Ethics Committee of the Federal University of Bahia (UFBA) (No. 2.857.836). The parents and/or legally responsible person received detailed information about the objective of the study and signed the free informed consent form. The data were analyzed using the IBM SPSS Statistics 25® program (Statistical Package for the Social Science). Summary statistics were used for descriptive analysis of the data. Categorical variables are reported as absolute and relative frequency, and continuous variables as mean and standard deviation (SD) or median.
Results
Most of the 632 children evaluated were girls (n = 317, 50.2%). Age ranged from 6 to 36 months and the mean age of the participants was 18.45 months (SD = 8.91). Regarding skin color, 53.8% of the children were brown and 30.6% were black. Almost half the mothers (47.5%) had complete high school and only 8.7% had completed higher education. Most fathers and mothers had some occupational activity, while 45.2% carried out only household activities. Regarding household income, 273 households received one minimum wage; 45.3% received social welfare (Bolsa Família Program). Analysis of the mother’s age showed that 42.7% were between 21 and 30 years old and 21.2% were younger than 21 years (Table 1). With respect to general health of the mothers and prenatal care, most mothers (65.4%) underwent dental prenatal care. The characteristics of prenatal health care are shown in (Table 2). Four (0.6%) of the 632 participants did not consider it important to take care of their child’s teeth and one (0.2%) was indifferent. Most parents/caregivers (72.5%) reported to have received instructions about oral health care; 64.8% received information from the doctor/nurse and 41.9% from a dentist/oral health technician/oral health agent.
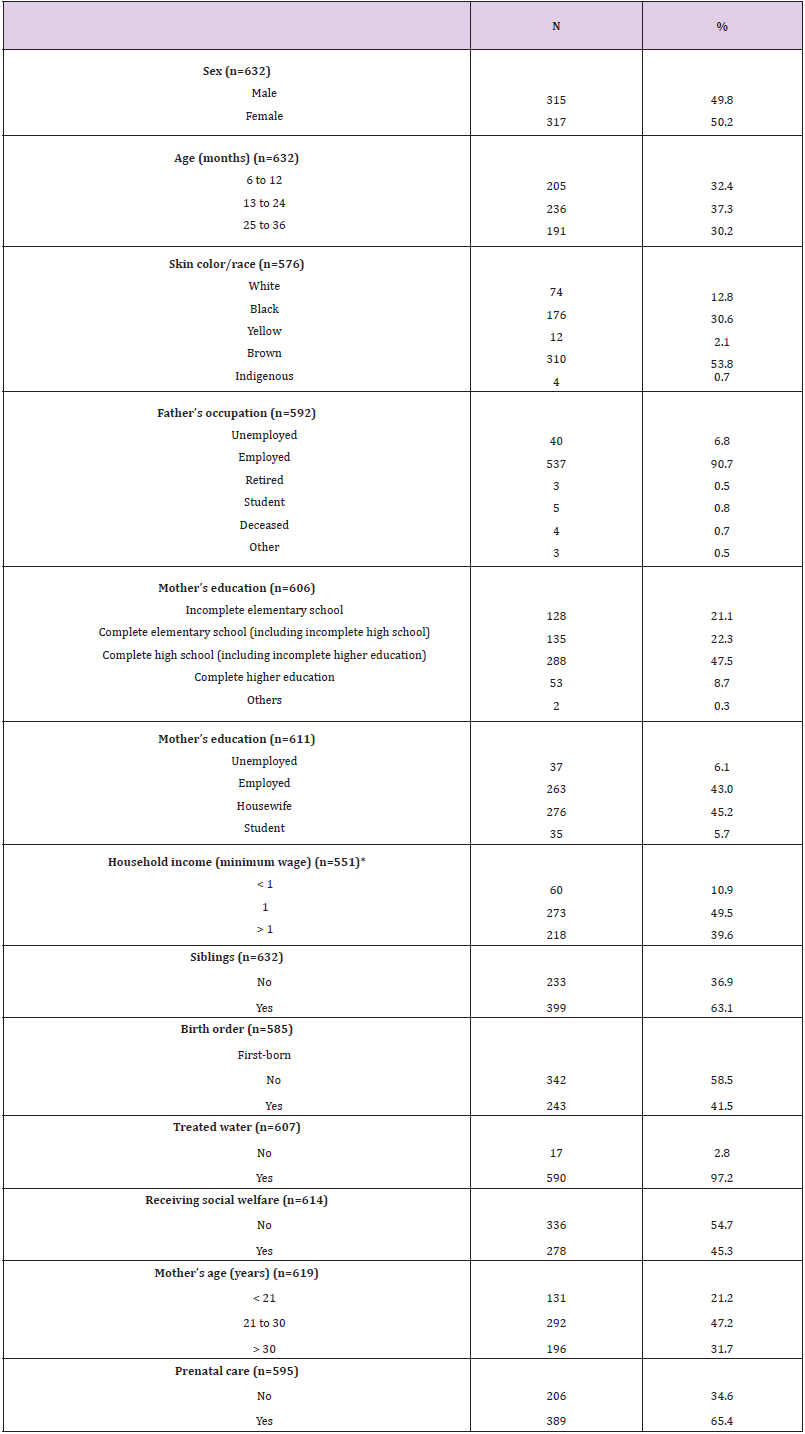
Table 1: Sociodemographic characterization of the participants aged 6 to 36 months from Salvador, BA, 2018 (n=632).
Note: Brazilian minimum wage: ±U$ 252.00.
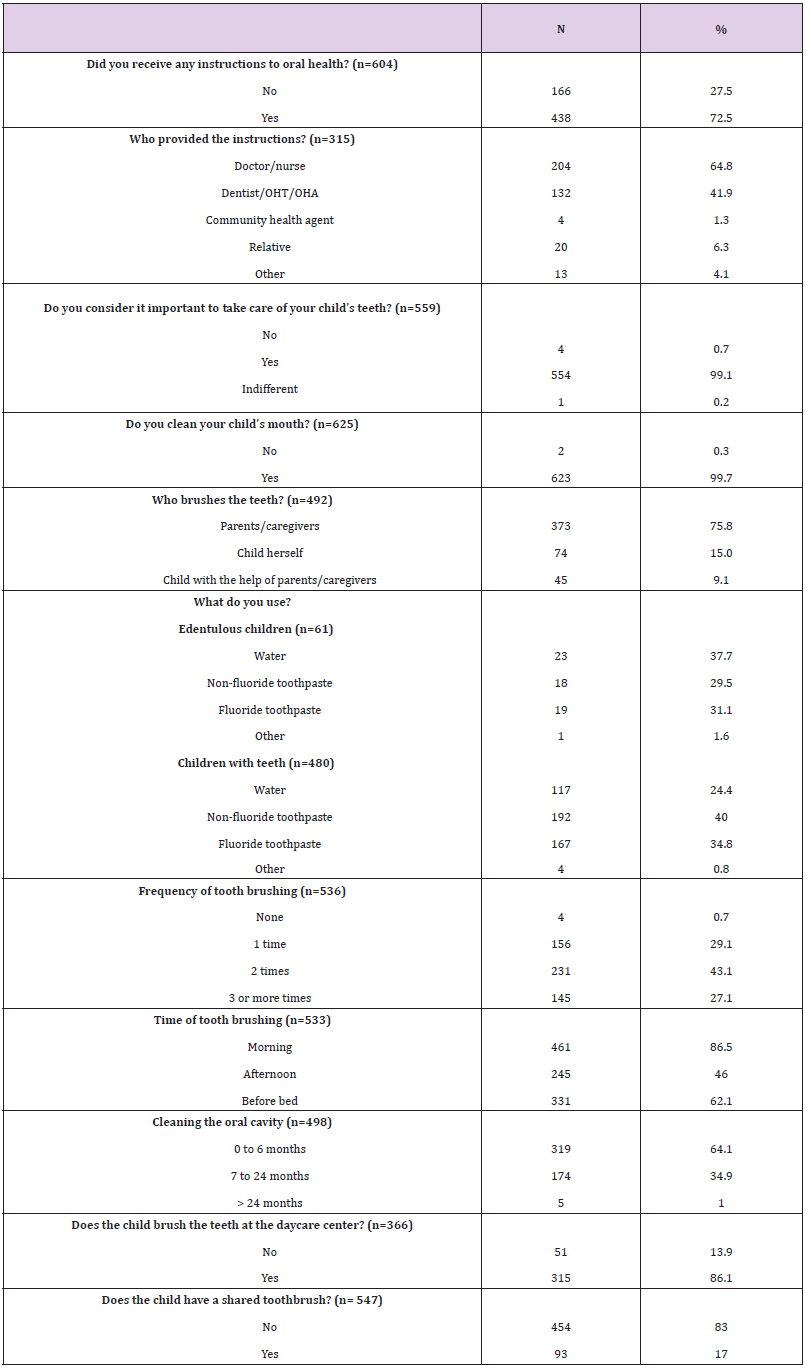
Table 2: Characterization of oral health care in the participants aged 6 to 36 years from Salvador, BA, 2018 (n=632).
Note: OHT: oral health technician; OHA: oral health auxiliary.
When asked about who cleaned the oral cavity of the child, 15% answered that the child herself does it. Regarding the question what was used for cleaning the oral cavity, only water was used in 37.7% of edentulous children and non-fluoride toothpaste in 40% of children who had teeth. About 70.2% of children cleaned the oral cavity two or more times per day, mainly in the morning (86.5%) and at night (62.1%). Cleaning of the oral cavity was started before 6 months of age in 64.1% of the children. The percentage of children who brushed their teeth at the daycare center was 86.1% and 17% of the children shared their toothbrush. (Table 3) shows the results regarding adequate oral hygiene in edentulous children and children with teeth. Inadequate oral hygiene was observed in 76% of edentulous children and in 77.7% of children with teeth.
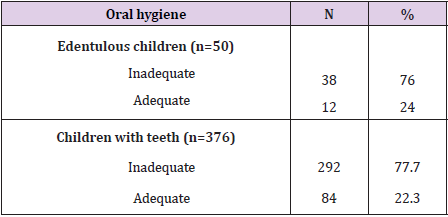
Table 3: Characterization of adequate oral hygiene in the participants aged 6 to 36 years from Salvador, BA, 2018 (n=632).
Discussion
The main results showed that most children were brown and black girls with a mean age of 18.45 months. In addition, 72.5% of the participants received oral hygiene instructions, 99.1% considered it important to take care of their child’s teeth, and 99.7% reported to perform oral hygiene. However, only 34.8% of the children used fluoride toothpaste and 17% shared the toothbrush. According to the criteria of the American Academy of Pediatric Dentistry (AAPD), early childhood caries is defined as the presence of one or more decayed teeth (cavitated or non-cavitated lesions), missing teeth due to caries, or filled tooth surface in any primary tooth of children younger than 6 years of age [21]. In addition to traditional risk factors, sociodemographic characteristics of the parents/ caregivers, especially education level, profession, household income and number of children, have also been associated with early caries [14,15]. Early childhood caries can be avoided by adopting better oral hygiene habits such as tooth brushing twice a day after eruption of the first tooth, use of fluoride toothpaste and regular visits to the dentist, as well as adequate eating habits such as a reduction in sugar intake [14,15,22].
Brown or black skin color predominated in the present study. Studies have shown significant differences in oral health among different racial groups and that skin color influences social, cultural and behavioral patterns [23]. The culture of each person can interfere with his/her motivation, responses to health care, and adoption of health care practices [24]. The household income was one minimum wage in about half the sample of this study, a fact limiting the possibilities of oral care in these children when compared to children from higher socioeconomic status families. Within this context, studies have shown that children from low socioeconomic status families have more carious teeth than children of medium or high socioeconomic status [25]. Supporting this evidence, Sun et al. demonstrated a gradual reduction in early childhood caries with increasing annual household income [15]. About 2.8% of the sample had no access to treated water. Although this percentage is low, water treatment is a preventive measure that should be adopted in all residences since exposure to fluoridated water is effective in preventing caries. In this respect, the continuous supply of fluoride at low doses prevents biofilm formation and incipient caries lesions [17,18].
Mothers are known to be the primary promoters of oral hygiene and eating habits of children. In addition, mothers who have completed high school or have a higher education degree have better oral health knowledge. It is therefore expected that the higher the education level of the parents, the better the information they will pass on to their children [26]. Sakalauskiene et al. observed that a higher level of schooling of the parents, especially maternal education, was associated with a lower prevalence of early childhood caries [27]. Most mothers had received prenatal care. This practice plays an important role in the prevention of early childhood caries as the mothers receives dental treatments and information about oral care of her child [25]. It is therefore of particular relevance that mothers are aware of the importance of oral health for them and for their children.
Although most participants reported cleaning their child’s mouth, more than a quarter received no instructions on oral care. Providing increased information about oral health care practices has been shown to significantly reduce early childhood caries [28]. Among the participants who received instructions, the doctor/ nurse provided the information in most cases, demonstrating the importance of an expanded team for the oral health care of children. Among edentulous children, water was used to clean the oral cavity in 37.7%, while fluoride or non-fluoride toothpaste was used in the remaining cases. Controversy exists regarding oral hygiene in edentulous children, which can be done in two ways: after breastfeeding with a rubber finger brush or gauze soaked in clean water. Jurgensen et al. defend that infants receiving oral hygiene at this stage have a lower risk of developing oral diseases, particularly oral candidiasis, experience less discomfort during eruption of the first teeth, and exhibit a lower incidence of early childhood caries [29].
According to the literature, preventive measures of early childhood caries should promote supervised tooth brushing with fluoride toothpaste after eruption of the first tooth, as fluoride plays an important role in the remineralization process of enamel [15,17]. In the present study, 34.8% of children with teeth used nonfluoride toothpaste, i.e., the parents/caregivers were not properly oriented towards the importance of using fluoride toothpaste. In the present study, 43.1% of the children brushed their teeth twice a day. This percentage is lower than expected since studies recommend tooth brushing to be done at least twice a day [14,22]. Despite the observation that the majority of parents/caregivers brushed the child’s teeth, almost one-fourth of the children brushed their own teeth. The literature shows that children under 3 years of age do not have a sufficiently developed degree of fine motor skills to autonomously brush their teeth [14]. About 9.1% of the children brushed their teeth with the help of their parents/caregivers. The latter are responsible not only for brushing the child’s teeth in order to increase the effectiveness of cleaning and plaque removal, but also for supporting and encouraging them to do so up to 6 to 7 years of age, when the child has acquired the ability to write [14,25].
Individual analysis of the variables used for the classification of “adequate oral hygiene” showed that 37.7% of edentulous children used water, 78.8% washed the oral cavity at an adequate frequency, and brushing was performed by the parents/caregivers in 76.4% of the children. However, when the three variables were summed, only 24% of edentulous children exhibited adequate oral hygiene. Among children with teeth, 34.8% correctly used fluoride toothpaste, 69.7% brushed their teeth at the appropriate frequency, and in 86% tooth brushing was performed by the adequate person. The sum of the three variables showed adequate oral hygiene in 22.3% of children with teeth. These data highlight the need to raise the awareness of parents that adequate oral hygiene is not characterized by a single measure but by a set of practices that have to be performed simultaneously, in agreement with the findings of other studies [3,30].
Conclusion
Most of the children aged 6 to 36 years from the municipality of Salvador received oral care instructions and reported to perform oral hygiene. However, oral hygiene habits are not well incorporated since many children do not use fluoride toothpaste and some children share the toothbrush. The measures for disease prevention and oral health promotion endorsed by the care practices of USF have the potential to promote healthier oral hygiene habits in early childhood with the aim of improving the results found in this study and ensuring adequate oral care practices of the child.
References
- Segre M, Ferraz FC (1997) O conceito de saú Revista de Saúde Pública 31: 538-542.
- Gil Montoya JA, de Mello AL, Barrios R, Gonzalez Moles MA, Bravo M, et al. (2015) Oral health in the elderly patient and its impact on general well-being: a nonsystematic review. Clinical interventions in aging 10: 461-467.
- Souza LR, Teixeira NM, Abreu TR, Oliveira CAS, Zocratto KBF, et al. (2017) Maternal knowledge regarding baby's oral health care. Odont Clin Cient Recife 16(4): 275-280.
- (2011) Ministry of Health. Department of Health Care. Department of Primary Care. National Coordination of Oral Health. SB Brasil 2010. National Oral Health Survey. Main Results. Brazil.
- Workie MS, Belay DB (2019) Bayesian model with application to a study of dental caries. BMC oral health 19(1): 4.
- Sanguino SM, Dhepyasuwan N, Church A, Dabrow S, Serwint JR, et al. (2017) Oral Health Promotion During Well Visits. Clinical pediatrics 56(10): 894-901.
- Alhabdan YA, Albeshr AG, Yenugadhati N, Jradi H (2018) Prevalence of dental caries and associated factors among primary school children: a population-based cross-sectional study in Riyadh, Saudi Arabia. Environmental health and preventive medicine 23(1): 60.
- Anil S, Anand PS (2017) Early Childhood Caries: Prevalence Risk Factors and Prevention. Frontiers in pediatrics 5: 157.
- Zhu C, Yuan C, Ao S, Shi X, Chen F, et al. (2018) The Predictive Potentiality of Salivary Microbiome for the Recurrence of Early Childhood Caries. Frontiers in Cellular and Infection Microbiology 8: 423.
- Salci MA, Maceno P, Rozza SG, Silva DMGVd, Boehs AE, et al. (2013) Health education and its theoretical perspectives: some reflections. Text & Context Nursing 22: 224-230.
- Anopa Y, Mc Mahon AD, Conway DI, Ball GE, McIntosh E, et al. (2015) Improving Child Oral Health: Cost Analysis of a National Nursery Toothbrushing Programme. PloS one 10(8): e0136211.
- Kumar S, Kroon J, Lalloo R (2014) A systematic review of the impact of parental socio-economic status and home environment characteristics on children's oral health related quality of life. Health and quality of life outcomes 12: 41.
- Ghaffari M, Rakhshanderou S, Ramezankhani A, Noroozi M, Armoon B, et al. (2018) Oral Health Education and Promotion Programmes: Meta-Analysis of 17-Year Intervention. Int J Dent Hyg 16(1): 59-67.
- Shaghaghian S, Zeraatkar M (2017) Factors Affecting Oral Hygiene and Tooth Brushing in Preschool Children, Shiraz Iran. Journal of dental biomaterials 4(2): 394-402.
- Sun HB, Zhang W, Zhou XB (2017) Risk Factors associated with Early Childhood Caries. The Chinese journal of dental research: the official journal of the Scientific Section of the Chinese Stemmatological Association (CSA) 20(2): 97-104.
- Turska Szybka A, Gozdowski D, Olczak Kowalczyk D (2014) Impact of individual health-oriented parent education on eating and hygienic habits, oral hygiene level, and dentition condition in children with high risk of caries. Developmental period medicine 18(2): 233-240.
- Carey CM (2014) Focus on fluorides: update on the use of fluoride for the prevention of dental caries. The journal of evidence-based dental practice 14: 95-102.
- Cruz M, Narvai PC (2018) Caries and fluoridated water in two Brazilian municipalities with low prevalence of the disease. Rev Saude Publica 52: 28.
- Watanabe M, Wang DH, Ijichi A, Shirai C, Zou Y, et al. (2014) The influence of lifestyle on the incidence of dental caries among 3-year-old Japanese children. International journal of environmental research and public health 11(12): 12611-12622.
- Daly JM, Levy SM, Xu Y, Jackson RD, Eckert GJ, et al. (2016) Factors Associated with Parents' Perceptions of Their Infants' Oral Health Care. Journal of primary care & community health 7(3): 180-187.
- Ballantine JL, Carlson JC, Ferreira Zandoná AG, Agler C, Zeldin LP, et al. (2018) Exploring the genomic basis of early childhood caries: a pilot study. International Journal of Paediatric Dentistry 28(2): 217-225.
- Ni L, Tang R, He T, Chang J, Li J, et al. (2017) Clinical effect of a manual toothbrush with tapered filaments on dental plaque and gingivitis reduction. American journal of dentistry 30(5): 272-278.
- Chiapinotto FA, Vargas Ferreira F, Demarco FF, Correa FO, Masotti AS, et al. (2013) Risk factors for gingivitis in a group of Brazilian schoolchildren. Journal of public health dentistry 73(1): 9-17.
- Tiwari T, Albino J (2017) Acculturation and Pediatric Minority Oral Health Interventions. Dental clinics of North America 61(3): 549-563.
- Wagner Y, Heinrich Weltzien R (2017) Risk factors for dental problems: Recommendations for oral health in infancy. Early human development 114: 16-21.
- Begzati A, Bytyci A, Meqa K, Latifi Xhemajli B, Berisha M, et al. (2014) Mothers' behaviours and knowledge related to caries experience of their children. Oral health & preventive dentistry 12(2): 133-140.
- Sakalauskiene Z, Machiulskiene V, Murtomaa H, Vehkalahti MM (2015) Satisfaction with dental care and its role in dental health-related behavior among Lithuanian university employees. Oral health & preventive dentistry 13(2): 113-121.
- Kressin NR, Nunn ME, Singh H, Orner MB, Pbert L, et al. (2009) Pediatric clinicians can help reduce rates of early childhood caries: effects of a practice-based intervention. Medical care 47(11): 1121-1128.
- Jurgensen N, Petersen PE (2009) Oral health and the impact of socio-behavioral factors in a cross-sectional survey of 12-year old school children in Laos. BMC oral health 9: 29.
- Monte DO, Lima PR, Machado RMA, Correia AA (2015) Awareness of the hygiene of the Brazilian population. Cien Biol Health Ten 2(2): 53-60.
