 Research Article
Research ArticleAbstract
The Homeless population is the most socioeconomic underprivileged community in the United States. Cardiovascular complications are one of the leading causes of death among homeless individuals. This study highlights the major risk factors of hypertension among the homeless community in the Orlando metropolitan area, in order to provide solutions and to modify associated risk factors. Adult homeless individuals (N=167) were randomly selected during daily lunch shares at St. George Orthodox Church, Orlando Florida. Each consented participant completed a survey with inquiries about demographic, lifestyle and hypertension related risk factors. Blood pressure was measured twice using an automatic Welch Allyn Connex ProBP 2400 digital device and the readings average was calculated. The Body Mass Index (BMI) was also calculated according to the World Health Organization (WHO) criteria. Average age of participants was 42.3 ± 11 years, and 83% were men. The overall prevalence of hypertension among participants was 52% (87 out of 167). The prevalence of hypertension among individuals who reported to be homeless over one year was 73% (38 out of 52), compared to only 51.3% among those with less than one year. Among diabetic homeless, 70% suffers from hypertension. The prevalence of hypertension among smokers was 51% (48 out of 95), while hypertension according to BMI group was significantly higher in both overweight and obese groups compared to individuals with normal BMI. Hypertension was significantly prevalent among homeless receiving no assistance (75.67%) compared to those receiving both financial and social assistance (47.61%). However, financial assistance had a major effect on lowering hypertension prevalence in comparison to social assistance (58.62% and 74.41%, respectively). In conclusion, hypertension is prevalent among Orlando homeless cohort and it has surpassed the national average. Clearly, social and financial services seem to lower hypertension prevalence among homeless individuals receiving benefits. The outcome of the study supports data from other countries offering affordable and accessible health care services, and certainly, it renews the call for more resources to help the homeless communities.
Keywords: Communicable Diseases; Cardiovascular Disease; Hypertension; Blood Pressure; Diastolic Blood Pressure
Abbreviations: WHO: World Health Organization; BMI: Body Mass Index; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure
Introduction
Homelessness is defined as a condition of people living without any regular nighttime residence [1]. As of 2017, there were around 550,000 homeless individuals in the United States, which is considered 0.17% of the total population [1,2]. Studies addressing the health risks of homelessness are very limited. Homeless individuals are prone to developing chronic disease conditions, communicable diseases and substance abuse [3-5]. Since there is a strong correlation between socioeconomic status and health, it is not surprising that homeless individuals are facing a heavy disease burden, which requires a distinctive approach to fulfill their health care needs [6]. Among the most common chronic illnesses affecting homeless people is cardiovascular disease [7]. However, the risk factors associated with its manifestations are generally unidentified [3]. Most of homeless people are lacking health insurance, which results in deadly consequences of cardiovascular disease specifically [3]. For instance, hypertension is estimated to affect between 18% to 41% of the homeless population [8]. Hypertension has been found to be a leading risk factor for death worldwide [9,10]. Consequently, homeless individuals have an average life expectancy of 42 to 52 years old, almost 30 years less than the average American [8].
This study was designed to determine the prevalence of hypertension among the homeless community of downtown Orlando area, where 1500 individuals are estimated to be homeless. Additionally, we wanted to identify certain risk factors inducing the development of hypertension among these individuals. Ultimately, this could help educating the public about this issue, which will potentially assist the city to develop more effective and efficient solutions, that they might not have been considered earlier.
Materials and Methods
Enrollment of Study Participants
All participants in this study were self-identified as homeless adults residing in Orlando Downtown, Florida. All participants have consented to be enrolled in the study following an approved Institutional Review Board from the University of Central Florida (IRB00001138). All participants were interviewed and selected for the study following approved inclusion/exclusion criteria defined in the IRB protocol and the consent form. Exclusion criteria includes those who were under the age of 18 years old, pregnant women, had permanent housing, had received mastectomies, and had consumed alcohol on that day. Additionally, we conducted a brief visual check to ensure that participants’ left arm were not amputated and that they were not suffering from any present ablations or cuts that may lead to complications if the blood pressure was measured. To conduct the study effectively, we aimed to recruit a sizeable and representative sample of the Orlando homeless community. Thus, with the permission of the St. George Orthodox Church (Orlando, Florida), we conducted the study on their property during their daily food shares. Recruitment took place between January 22nd, 2018 and February 26th, 2018.
Each participant was asked to complete a survey form, which included questions in regard to smoking, alcohol consumption, diet habits, veteran status, diabetes history, high blood pressure history, financial support, social support, current medications, cause of homelessness, duration of homelessness, weight, and height. The Body Mass Index (BMI) was calculated according to the World Health Organization (WHO) criteria. Blood pressure measurement Blood pressure was measured twice in one setting, by using an automatic Welch Allyn Connex ProBP 2400 digital device. Each participant was seated, and blood pressure sanitized cuff was securely wrapped around the left arm, then Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP) were documented accordingly.
Statistical Analysis
First, we quantified the responses to each survey question, which indicated the prevalence of certain factors, behaviors, or characteristics within the sample that effectively represents the Orlando homeless community. Data are expressed as mean ± standard error of the mean by using graphpad prism®. Two tailed student’s t-test was used. The difference between samples and controls was considered statistically significant at a level of *P<0.05. In order to compare between the homeless population and the nonhomeless population (derived from other studies), a Z-Test for two population proportions was conducted to determine if there was a statistically significant difference.
Results
Presence of Hypertension Among Homeless Population
Of over 200 individuals were interviewed, 167 agreed to participate in this study. Demographics of study participants are listed in Table 1. The average age of participants was 42.3 ± 11 years, and 83% were men. Physical and social characteristics of study participants are listed in Table 2. Evaluated based on a mean systolic blood pressure of higher than 130 mm Hg or a mean diastolic blood pressure of higher than 80 mm Hg, 52% (87 out of 167) of homeless individuals had hypertension. Additionally, 33 (20%) individuals were in a prehypertension stage (SBP 120–129 and DBP <80 mm Hg). Surprisingly, only 7 individuals (4%) out of those were aware of their hypertension and currently taking antihypertensive medication. The prevalence of hypertension among individuals who reported to be homeless over one year was 73% (38 out of 52), which is significantly higher than individuals who were homeless for less than a year (51.3%) (Figure 1A).
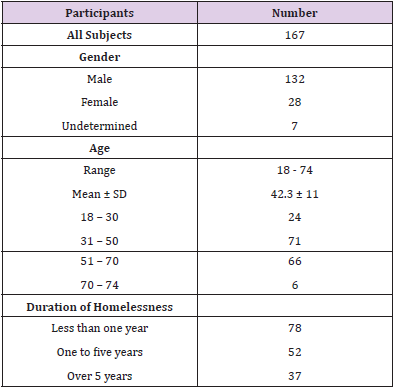
Table 1: Participant Demographics.
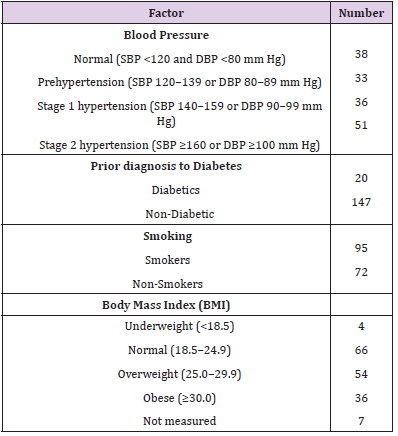
Table 2: Physical and Social Characteristics of Study Participants.
Effects of Diabetes, Smoking, Bmi And Age on Hypertension Prevalence
The prevalence of self-reported diabetic patients among the homeless population was 12% (20 out of 167), 70% (14 out of 20) of those patients were found to have hypertension (Figure 1B). The prevalence of cigarette smoking among homeless population was 45% (95 out of 167). The prevalence of hypertension among those was 51% (48 out of 95). The BMI of 54% (90 out of 167) of homeless individuals met WHO criteria for being overweight or obese (BMI ≥ 25). On the other hand, only 4 individuals (2.4%) were underweight (BMI < 18.5). The presence of hypertension according to BMI group was significantly higher in both overweight and obese groups compared to normal BMI group (Figure 1C). Individuals who were over the age of 50, had significantly higher prevalence of hypertension compared to those under 50 (69.4% vs 48.42%, respectively), although hypertension is still significantly prevalent within each group (Figure 2).
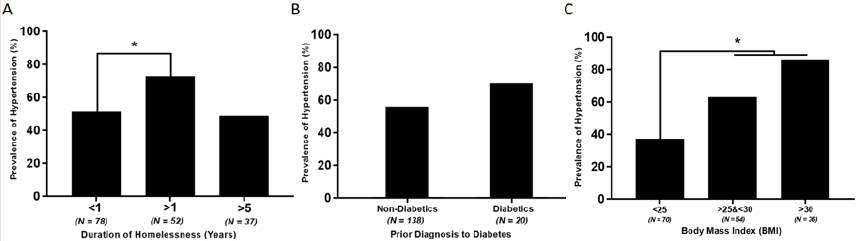
Figure 1: Effect of homelessness duration (A), Body mass index (B) and Prior diagnosis to diabetes (C) on hypertension prevalence among homeless individuals.
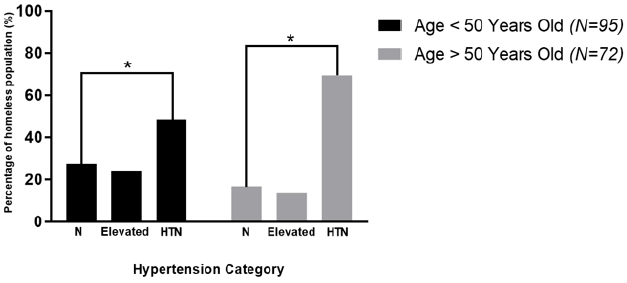
Figure 2: Distribution of hypertension categories according to age groups.
Hypertension Prevalence Among Individuals Receiving Financial and Social Assistance
Out of 167 surveyed individuals, 29 (17.4%) have reported to receive financial assistance from designated authorities, while 43 (25.7%) have reported to receive social assistance. Additionally, 21 (12.57%) have reported to have both social and financial assistance, while 74 individuals were not receiving any assistance. Hypertension was significantly prevalent among individuals receiving no assistance (75.67%) compared to individuals receiving both financial and social assistance (47.61%). However, financial assistance had a major effect on lowering hypertension prevalence in comparison to social assistance, since it was 58.62% and 74.41%, respectively (Figure 3).
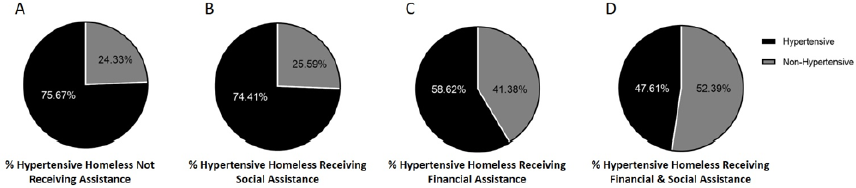
Figure 3: Prevalence of hypertension among homeless individuals receiving financial or social assistance.
Discussion
Several research studies have focused on elucidating the socioeconomic discrepancies in prevalence of risk factors leading to cardiovascular disease [11,12,13]. Nevertheless, a small attention has been paid to study those risks among the homeless population, which represents the most socioeconomic underprivileged community in the United States [14,15]. This study, which is one of the first to assess risk factors of hypertension among homeless individuals in Orlando metropolitan area, demonstrates high prevalence of major risks in this community. The prevalence of hypertension was significantly higher among the homeless population regardless of age group, although it was higher in individuals over 50 compared to those under 50 years old. It is noteworthy to mention that only 7 individuals were aware of their hypertension situation and they were taking medications accordingly. This indicates an evidence of inadequate diagnosis and treatment of hypertension in this community. Additionally, only a small group of individuals (20 out of 167) has self-reported their diagnosis of diabetes, which shows that diabetes might be underdiagnosed as well. Moreover, cigarette smoking, alcoholism and obesity were all prevalent among homeless individuals, which imposes additional risk factors for cardiovascular disease in general. We should also bear in mind that financial and social assistance play a major role in decreasing the prevalence of hypertension in this population as our results indicate. Overall, Hypertension is prevalent among the Orlando homeless metropolitan community, which surpasses the national average. This observation might be attributed to high prevalence of main cardiovascular risk factors such as smoking and drug abuse among homeless individuals, in addition to hurdles to overcome those factors [16,17]. Furthermore, the diet of homeless individuals is usually high in saturated fats and insufficient in essential nutrients, which leads to abnormalities in their lipid panel [7,18]. The study shows that social and financial services seem to lower hypertension prevalence among homeless individuals receiving the benefits. The study supports data from other countries offering affordable and accessible health care services. Specifically, our study provides a trend like data reported in Canada where hypertension prevalence was found to be only 35% among homeless population in the city of Toronto [19]. Canada provides affordable and accessible health care services to all residents including homeless individuals. We strongly believe that the prevalence of hypertension is much higher in other major cities especially those with harsher climate conditions. We plan to do a larger scale study on homeless communities residing in other major metropolitan cities and during different times of the year. Our study renews the call for more resources to help the homeless communities including development of more intervention programs to reduce smoking, and alcohol and substance abuse.
Significance for Public Health
Hypertension is found to be prevalent among Orlando homeless community and it has exceeded the national average in the United States. Additionally, social and financial aids seem to decrease the prevalence of hypertension among homeless individuals receiving these benefits. The outcome of the study supports data from other countries offering affordable and accessible health care services, and certainly, it renews the call for more resources to help the homeless communities.
Acknowledgement
Sincere thank you to our team volunteers including Ahmad Odeh, Abdel-Rahman N. Naser, Abed El-Rahman S. Naser, Sarah Abdelhameed, James Overman, Anupa Thirmiya, Elizabeth Aguilar, Kayla Ferro, Ranya Awad, Corrine Haeberlin, Adrian Doddson, Iman Squires, Heather Issa, Theodora Meza, Bobak Manesh, and Elena Pham. Our thanks are also due to all the participants in our study and to the volunteers led by Chris Wilson at St. George Orthodox Church, Orlando, Florida.
Competing Interest
The authors declare that they have no competing interests.
Funding Sources
This study was supported, in part, by the Hearts for the Homeless project.
Availability of Data Materials: The datasets supporting the conclusions of this article are included within the article.
References
- Wright J (2017) Address unknown: The homeless in America. Routledge 1-220.
- Koh HK, O Connell JJ (2016) Improving health care for homeless people. Jama 316(24): 2586-2587.
- Bernstein RS, Meurer LN, Plumb EJ, Jackson JL (2015) Diabetes and hypertension prevalence in homeless adults in the United States: a systematic review and meta-analysis. American Journal of Public Health 105(2): e46-e60.
- Fazel S, Geddes JR, Kushel M (2014) The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations. The Lancet 384(9953): 1529-1540.
- Aldridge RW, Story A, Hwang SW, Nordentoft M, Luchenski SA, et al. (2018) Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. The Lancet 391(10117): 241-250.
- Hwang SW, Chambers C, Chiu S, Katic M, Kiss A, et al. (2013) A comprehensive assessment of health care utilization among homeless adults under a system of universal health insurance. American Journal of Public Health 103(S2): S294-S301.
- Szerlip MI, Szerlip HM (2002) Identification of cardiovascular risk factors in homeless adults. The American journal of the medical sciences 324(5): 243-246.
- Zlotnick C, Zerger S (2009) Survey findings on characteristics and health status of clients treated by the federally funded (US) Health Care for the Homeless Programs. Health & social care in the community 17(1): 18-26.
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, et al. (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The lancet 380(9859): 2224-2260.
- Kannel W B (1996) Blood pressure as a cardiovascular risk factor: prevention and treatment. Jama 275(20): 1571-1576.
- Sommer I, Griebler U, Mahlknecht P, Thaler K, Bouskill K, et al. (2015) Socioeconomic inequalities in non-communicable diseases and their risk factors: an overview of systematic reviews. BMC public health 15(1): 914.
- Leng B, Jin Y, Li G, Chen L, Jin N (2015) Socioeconomic status and hypertension: a meta-analysis. Journal of hypertension 33(2): 221-229.
- Cesaroni G, Forastiere F, Stafoggia M, Andersen Z J, Badaloni C, et al. (2014) Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. Bmj 348: f7412.
- Martens WH (2001) A review of physical and mental health in homeless persons. Public health reviews 29(1): 13-33.
- Weiser SD, Bangsberg DR, Kegeles S, Ragland K, Kushel MB, et al. (2009) Food insecurity among homeless and marginally housed individuals living with HIV/AIDS in San Francisco. AIDS and Behavior 13(5): 841-848.
- Ober K, Carlson L, Anderson P (1997) Cardiovascular risk factors in homeless adults. The Journal of cardiovascular nursing 11(4): 50-59.
- Connor SE, Cook RL, Herbert MI, Neal SM, Williams JT (2002) Smoking cessation in a homeless population: there is a will, but is there a way? Journal of General Internal Medicine 17(5): 369-372.
- Luder E, Ceysens Okada E, Koren Roth A, Martinez Weber C (1990) Health and nutrition survey in a group of urban homeless adults. Journal of the American Dietetic Association 90(10): 1387-1392.
- Lee TC, Hanlon J G, Ben David J, Booth G L, Cantor WJ, et al. (2005) Risk factors for cardiovascular disease in homeless adults. Circulation 111(20): 2629-2635.
