 Short Communication
Short CommunicationIntroduction
Laparoscopy has become the standard of care in many surgical interventions over the last two decades. Gaining access to the intraperitoneal space and establishing pneumoperitoneum remains a crucial step to be safely achieved during these procedures. Veress needle, open Hasson’s technique and Undervision trocars are currently the most common types used to enter the abdominal cavity [1]. Irrespective of the technique employed, the rate of visceral organs and vessels injuries ranges somewhere between 0.04% and 0.05% as demonstrated by large scale meta-analysis studies [2-5]. The mechanism of injury in trocars insertion will depend on 2 factors: the proximity of the intraabdominal structure and the surgeon’s driving force when inserting the trocar. Since the former cannot be controlled for, we decided to modify the latter in order to decrease the rate of injuries.
The relationship between Pressure, Force and Area is [6]:

This Pressure depends mainly on the nature of the surface one is dealing with. It acquires its characteristics from the chemical composition and properties of the elements making-up this surface. Whenever a surface’s resistance increases, the required Pressure to break through it will eventually increase. Consequently, over the same Area, a higher Force will be required to achieve this higher Pressure. While inserting a trocar, the Force required to break through the abdominal fascia, proportionally increases with the required Pressure measured by the trocar sensors. Thus, for the same Area, we postulated that making a very small incision in the abdominal fascia, using an 11 mm blade, will lead to Less Resistance, consequently Less exerted Pressure, consequently Less exerted Driving Force of entry, consequently Less rate of injury associated with higher entry Forces.

Material and Methods
Patients
Patients undergoing laparoscopic surgical interventions, between October 2016 and April 2017, were included in the study. Patients included have had no prior abdominal surgeries, and no umbilical or epigastric hernia on preoperative physical examination. 100 patients were assigned randomly and equally in 2 groups. The first group consisted of 50 patients, in whom pneumoperitoneum was established through a veress needle and then trocars were inserted, without incision of the abdominal fascia. The second group consisted of 50 patients in whom the abdominal fascia was incised, in a pinprick fashion, around 2-3 mm, with an 11 mm blade, prior to the insertion of the veress needle and trocars.
Methods
An infra-umbilical smiley incision was made, the fascia was incised or left intact, according to the patient’s random group assignment, the abdominal wall was lifted and veress needle inserted. After creation of the pneumoperitoneum, trocars were inserted in their respective sites, with or without incision of the fascia as well. 5, 10 and 15 mm trocars were used. All insertions were performed by the same operator using disposable, sharp trocars, with a conical tip (Figure 1). A 2 cm, circular transducer was constructed from piezoresistive material that changes its impedance as force is exerted on its surface. The transducer is connected by an interface box to a personal computer to record surface contact pressure digitally, continuously during trocar insertion. The transducer was positioned in the center of the operator’s palm such that each flat surface was in contact with either the hand or the top of the trocar. All insertions were performed by the same operator. No failed attempts were recorded (Figure 2).
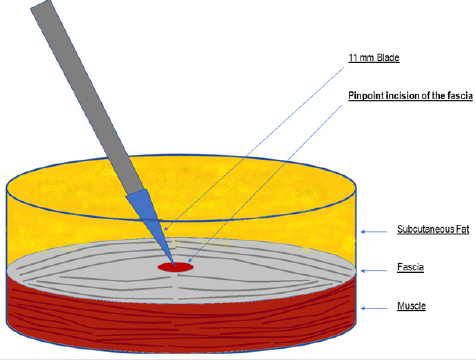
Figure 1: Pinpoint incision of the fascia with an 11 mm Blade was performed before Veress needle or Trocar insertion.
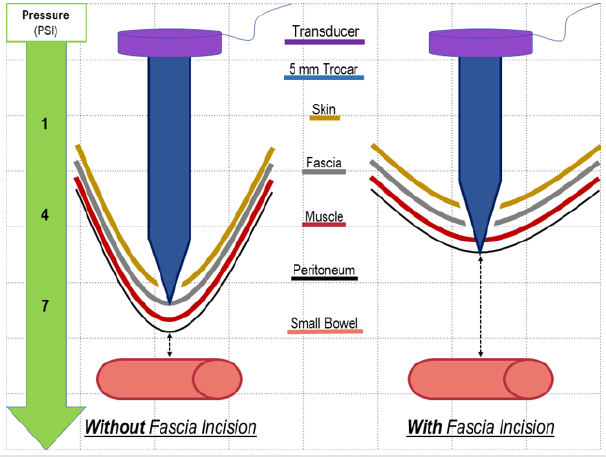
Figure 2: Trocar insertion Without vs With Fascia Incision.
Results
Of the 100 patients operated, there was no reported injuries. The recorded Pressures, while inserting either veress needles or trocars, were much lower whenever an incision of the abdominal fascia was done (Table I). Chart I, shows the difference between both groups.

Table 1: Mean recorded Pressure (in PSI), exerted while inserting veress needle and trocars, before and after incision of the fascia.
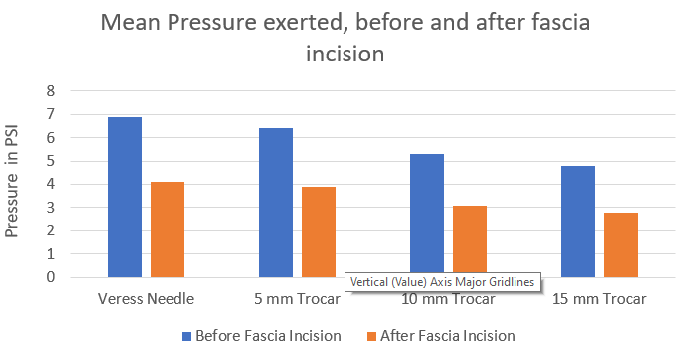
Chart 1: Mean recorded Pressure (in PSI), exerted while inserting veress needle and trocars, before and after incision of the fascia.
Discussion
The obtained results show a 40% decrease in the exerted Pressure while inserting the veress needle or any of the trocars when the abdominal fascia was incised. This decrease in Pressure clearly reflects a decrease in the driving Force as well. The ease of insertion, with a lower exerted driving Force, places the patient at minor risks of trocar-related injury [7]. It is true that in our series, none of the patients was injured in both groups. Thus, it is hard to compare “incision” versus “no incision” impact on decreasing the rate of injuries. However, the mere fact that the abovementioned technique allowed us to decrease the Driving Force, and we do know from the literature that the higher this force, the higher is the rate of injuries, we conclude that a pinpoint incision of the abdominal fascia, with an 11 mm blade, prior to veress needle or trocar insertion, decreases the risk for visceral organs and vessels injuries in laparoscopic surgeries.
Conclusion
Our study demonstrated a new technique, by which the Driving Force, associated with intraabdominal organs injury, can be minimized. An 11 mm blade, pinpoint incision of the abdominal fascia prior to Veress needle or Trocar insertion, could be easily and safely performed on regular basis if it decreases the risks of access into the abdominal cavity. Our small study can be an encouraging paper to further dwell on this technique, on a larger and broader scale. In our opinion, in a time experienced laparoscopic surgeon might not need to perform El Khoury Technique, it might reveal appealing in a teaching setting, to young surgeons and residents, whom trocars’ insertion force is not well controlled in the beginning of their career.
References
- Kassir R, Blanc P, Lointier P, Tiffet O, Berger JL, et al. (2014) Laparoscopic entry techniques in obese patient: veress needle, direct trocar insertion or open entry technique?. Obesity surgery 24(12): 2193-2194.
- Jiang X, Anderson C, Schnatz PF (2012) The safety of direct trocar versus Veress needle for laparoscopic entry: a meta-analysis of randomized clinical trials. Journal of Laparoendoscopic & Advanced Surgical Techniques 22(4): 362-370.
- Ahmad G, O Flynn H, Duffy JM, Phillips K, Watson A (2012) Laparoscopic entry techniques. Cochrane Database Syst Rev 15(2).
- Champault G, Cazacu F, Taffinder N (1996) Serious trocar accidents in laparoscopic surgery: a French survey of 103,852 operations. Surgical laparoscopy and endoscopy 6(5): 367-370.
- Schäfer M, Lauper M, Krähenbähl L (2001) Trocar and Veress needle injuries during laparoscopy. Surgical endoscopy, 15(3): 275-280.
- Halliday D, Resnick R, Walker J (2010) Fundamentals of Physics, Chapters 33-37. John Wiley & Sons
- Kelty CJ, Super PA, Stoddard CJ (2000) The driving force in trocar insertionrid. Surgical endoscopy 14(11): 1045-1046.
