 Case Report
Case ReportAbstract
Objectives: Complex regional painful knee syndrome (SRDC) type I is a pathology with many different origins and involves heavy physical and psychological repercussions. Its rehabilitation care is still poorly studied, although it is essential. Soft practices are beneficial when rehabilitating osteoarticular pathologies similar to the SRDC. It is therefore interesting to see the impact of such practices on the SRDC on both functional abilities and quality of life.
Material and Methods: Three subjects with knee algodystrophy participated in the program at a rate of 3x1h/week for 4 weeks. All sessions were individual. Lower limb muscle strength, joint amplitude, walking quality and speed, as well as kinesiophobia, quality of life, self-esteem and perceived pain were studied.
Results: Thanks to this program, all functional abilities have been improved for all 3 subjects. The rate of kinesiophobia decreased in two of the three subjects, physical and mental qualities of life and self-esteem were increased in all subjects, and perceived pain decreased in all three subjects.
Conclusion: This rehabilitation protocol seems to improve all the physical and psychological qualities altered by the complex regional painful knee syndrome.
Keywords: Complex regional painful syndrome; Algodystrophy; Gentle Gymnastics; Quality of Walking; Quality of Life; Rehabilitation
Abbreviations: SRDC: Regional Painful Complex Syndrome; PSPP: Physical Self-Perception Profile
Introduction
Regional Painful Complex Syndrome (SRDC), also known as algoneurodystrophic syndrome, is a condition that refers to persistent chronic pain that is disproportionate to the initial trauma or injury [1], sensory and vascular alterations, and often results in a physical disability with profound psychological impact [2]. Pain is usually increased by movement, joint pressure, and specific postures. These joint pains cause a decrease in muscle strength and also balance disorders as well as alterations in the quality of walking [3].
The pain and disability inherent in this pathology can lead to high anxiety and even depression, which can lead to passive coping strategies (due to increased pain through movement), a significant decrease in self-esteem, quality of life [4]. and the emergence of fear of movement due to pain: kinesiophobia [5].
The SRDC is mainly managed by physiotherapy, with passive mobilization of the joint concerned to avoid causing pain. To the best of our knowledge, there are no study about the management accompanied with physical activity. However, there are a number of gentle practices (Tai-chi and Pilates) used in other osteoarticular diseases (rheumatoid arthritis, osteoporosis, arthritis and/or fibromyalgia) [6], and are recognised for their beneficial effects on health. They are based on intertwining dynamic forms and slow, calm movements [7,8]. Moreover, these methods have a positive effect on balance and walking ability, thus improving daily life. Within the framework of adapted physical activities (APA), it is possible to work according to different objectives, with the intention of fighting kinesiophobia [9] Goubertet al. 2007), improving the quality of walking and also fighting sedentary lifestyles [10].
Our study therefore focuses on the effects of gentle practice (Tai-Chi and Pilates) on patients with SRDC. We hypothesise that this program could improve joint amplitude and walking quality Lange et al. (2000) [11], but also reduce pain and kinesiophobia and finally improve quality of life and self-esteem.
Materials and Methods
Subjects
Three subjects (two women, one man) with a SRDC located at the knee were followed during the implementation of an adapted gentle gymnastics protocol. The characteristic of the subjects is described below.
Subject 1: Female, 43 years old, 162 cm, 97 kg (BMI: 36.96). Following a rupture of the anterior cruciate ligaments of the right knee, operated on in March 2016, she developed symptoms of SRDC type 1, confirmed in December 2016. She has been in physiotherapy since December 2016 and in APA since February 2017.
Subject 2: Female, 43 years old, 160 cm, 57 Kg (BMI: 22.27). She underwent anterior cruciate ligament surgery in her left knee in June 2014. After two scans, the Type 1 SRDC was diagnosed in June 2016. She has been cared for in physiotherapy and APA since December 2016.
Subject 3: Male, 47 years old, 178 cm, 106 Kg (BMI: 33.45). Algodystrophy was diagnosed in February 2017 following a right valgus tibial osteotomy in October 2016. He has been in physiotherapy since March 2017 and in APA since April 2017. At the beginning of the study, the subject used two crutches to move around.
All participants were informed of the nature of the study, testing protocols, possible risks or discomforts, and signed informed consent. Each subject could stop the study at any time. The anonymity of the subjects was guaranteed by coding. All procedures performed in this study were in accordance with the 1964 Helsinki declaration and its later amendments. As part of the professional degree (Master’s degree-Sport, Prevention Health and Well-being), this study was accepted and approved by the institutional board of the University of Orléans (France).
Protocol
Subjects participated in Tai-Chi and Pilates training for 1-hour sessions, 3 times a week, for 4 weeks (12 sessions). The first and last sessions were devoted to the various tests. The sessions were prepared in advance and then adapted according to the pain and shape of the subjects Rho et al. (2002). The objectives of the Tai-Chi sessions were to increase the amplitude for flexion and extension, but also to improve the representation of the body schematics, balance and coordination. Pilates sessions were designed to strengthen the muscles of the lower limbs and the entire postural sheath, to help rebalance while walking.
Data Collection
Pre- and post-care measures were carried out on the basis of physical and psychological tests. 10-metre walk test (TM10) [12]. used to assess the quality of walking. The recommendations for the optimal passage time of TM10 are 7.6 seconds for men and 8 seconds for women [13]. Sit to stand [14], is used to measure the strength of the lower limbs. For subjects aged between 19 and 49 years, the average time to complete the test is 6.2 +/- 1.3 seconds. This test is a simple and reproducible measure of lower limb function validated for patients with rheumatoid arthritis by Newcomer [15].
Joint Amplitudes: carried out using a goniometer (COMED, France). A complete knee flexion is 150°, a complete passive flexion does not exceed 135°.
Kinesiophobia: Measured using Tampa [16], includes 17 items, evaluated according to 4 levels of feelings ranging from “strongly disagree” (1) to “strongly agree” (4). A score greater than or equal to 40/68 is considered significant [17] and indicates that the person is afraid to perform certain movements or gestures, associated with subjective pain. This test was validated and translated into French by French and Roach [18].
Quality of life: measured using the SF-36 [19]. It includes 36 items evaluating a physical and a psychological dimension. For each dimension, the scores are added together, for a total of 100 points. A total of close to 100 points indicates a better quality of life.
Physical Self-Perception Profile (PSPP) by Fox and Corbin [20], validated in French (ISP-25) by Ninot et al. [21]. It consists of twenty-five questions, divided into six sub-scales to assess overall self-esteem, perceived physical value, endurance, athletic ability, physical appearance and strength. To answer, patients were asked to rate themselves on a Lickert scale from 1 (“strongly disagree”) to 6 (“strongly agree”). The closer the score is to 6, the higher the person’s self-esteem.
Subjective level of Pain: measured using the Visual Analog Scale [22]. It is in the form of a double-sided rule. The front part is addressed to the subject and is represented by a line, without graduation, ranging from “no pain” to “maximum pain imaginable”. The subject must point along this line, the level where his pain is best located. The level of pain is recorded on a scale from 0 to 10 on the back of the ruler. For a more objective assessment of pain, the patient is asked to focus only on the pain associated with the condition on the affected limb.
Results
All the results are presented in Table 1.
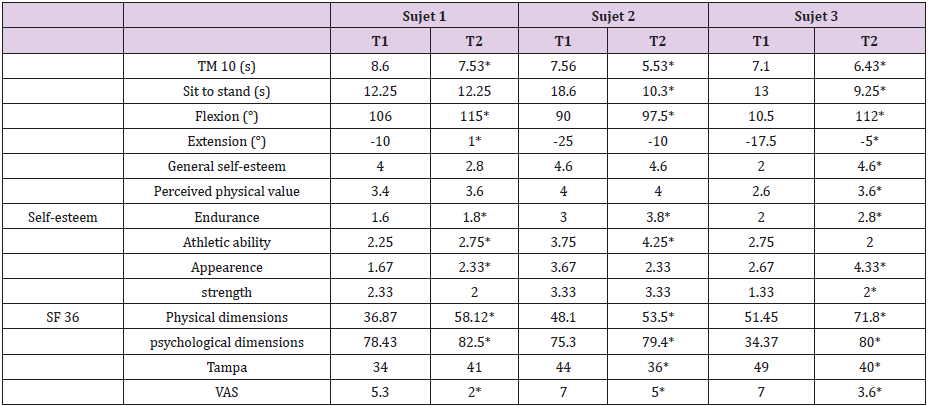
Table 1: Results obtained in the physical and psychological tests for each subject at the beginning (T1) and at the end of the treatment (T2).
TM10: 10-metre walk test. VAS: Visual Analog Scale
*significant score improvement between T2 et T1.
Subject 1
This patient has made little progress on tests measuring walking quality and lower limb strength, but her results are close to or above the recommendations. On the other hand, there was a gain in knee flexion and extension measurements. For psychological measures, overall, we have an increase in physical self-esteem except on the “overall self-esteem” sub-scale and the “strength” sub-scale. There has been an improvement in the quality of life on both dimensions. There is an increase in kinesiophobia in this patient, but she still reports a level of kinesiophobia that is close to normal. Finally, we observe a reduction in perceived pain.
Subject 2
This patient has made progress on all the physical parameters we evaluated, although her Sit to Stand result is still higher than recommended. The results obtained on psychological measures show an improvement in self-esteem (except for the “appearance” sub-scale), in both dimensions of quality of life, in kinesiophobia and in perceived pain. The results obtained on the kinesiophobia scale at the end of treatment are even below the critical score determined by the authors.
Subject 3
This patient has made progress on all the physical parameters we have assessed, although his Sit to Stand result remains above the recommendations. The results obtained on psychological measures show an improvement in self-esteem (except for the “sport competence” sub-scale), in both dimensions of quality of life, kinesiophobia and perceived pain. The results obtained on the kinesiophobia scale at the end of care are at the limit of the critical score.
Discussion
The Regional Painful Complex Syndrome is a pathology that is
still poorly defined, particularly in terms of management by APA
[23-25]. On the physical level, functional capacities are impaired by
joint limitation, pain, and muscle atrophy. Thus, the main functional
impact of the knee SRDC is on walking quality. These same factors
can also be at the origin of stopping walking Mazerat (2012). This
experiment is innovative, Thus, the lack of literature combining
adapted physical activities and complex regional painful syndrome
leads to questions about the efficiency of such a program, which
has never been tested before on this pathology. Unfortunately, no
comparative study can compare the results obtained.
The objective of this study was to evaluate the effects of a gentle
gymnastics program on the quality of walking, lower limb strength,
quality of life, perceived pain, self-esteem and kinesiophobia in
patients with SRDC. The benefits of these practices are increasingly
being studied, particularly in the context of the rehabilitation and
rehabilitation of osteo-articular diseases. Due to the specificity
of this pathology and the difficulty of recruiting enough subjects with identical joint disorders, a case study analysis was performed.
It allowed us to observe an overall improvement in the various
parameters measured for each subject, even if it is difficult to
project this result on a larger scale.
Nevertheless, this study shows an improvement in functional
parameters such as walking, strength and capacity in flexion and
extension (Table 1). Indeed, it was noted a significant change in gait
test performance (Table1), in accordance with the results obtained
by Lee et al. [26], as well as an improvement in joint amplitudes,
in flexion and extension, in accordance with the work of Wu et
al. [27]. These results suggest that appropriate physical activity
management based on gentle practice would improve range of
motion and walking quality. We have also obtained improvements
in quality of life measurements in accordance with the work of
Cruz-ferreira et al. [28], which demonstrated the positive effect of
pilate practice on quality of life. We also noted improvements in
self-esteem and perceived pain. However, the results obtained on
the kinesiophobia scale do not allow us to conclude that this type of
practice will have an effect on this phobic fear of movement, even
if two out of three patients seem to have reduced this fear [29-31].
Although promising, these results need to be confirmed by
other studies. Indeed, the few subjects included in this study, the
duration of the practice as well as the inter-individual differences
do not allow us to generalise our results. Moreover, the absence of
a control group does not allow us to affirm that these changes are
essentially due to soft practices. These promising results encourage
us to continue our research in this area.
References
- Bruehl S (2010) An update on the pathophysiology of complex regional pain syndrome. Anesthesiology 113(3): 713-725.
- Littlejohn GO (1998) Algodystrophy (reflex sympathetic dystrophy). Dans Oxford textbook of Rheumatology. Sous la direction de PJ Maddison, DA Isenberg, P Woo (Eds.), Glass. Oxford University Press Oxford pp. 1679-1689.
- Wasner G, Schattschneider J, Binder A, Baron R (2003) Complex regional pain syndrome--diagnostic, mechanisms, CNS involvement and therapy. Spinal Cord 41(2): 61-75.
- Tan EC, Van de Sandt-Renkema N, Krabbe PF, Aronson DC, Severijnen RS (2009) Quality of life in adults with childhood-onset of Complex Regional Pain Syndrome type I. Injury 40(8): 901-904.
- Khalfaoui S, Arabi H, Mehdaoui H, Alaoui Ismaili S, Jemmouj A (2014) Syndrome douloureux régional complexe type I: actualités de la prise en charge thé Maroc Rev Mar Rhum 27: 38-47.
- Wang C (2012) Role of Tai Chi in the treatment of rheumatologic diseases. Current Rheumatology Report 14(6): 598-603.
- Lan C, Lai JS, Chen SY, Wong MK (2000) Tai Chi Chuan to improve muscular strength and endurance in elderly individuals: a pilot study. Archives of Physical Medicine and Rehabilitation 81(5): 604-607.
- Kou J (2008) Tai-chi-chuan. Vanves: Marabout.
- Swinkels-Meewisse EJ, Swinkels RA, Berbeek AL, Vlaeyen JW, Oostendorp RA (2003) Psychometric properties of the Tampa Scale for kinésiophobie and the fear-avoidance beliefs questionnaire in acute low back pain. Man Ther 8(1): 29-36.
- INSERM (2015) Activité physique et prévention des chutes chez les personnes âgé Paris: Les éditions Inserm.
- Lange C, Unnithan VB, Larkam E, Latta PM (2000) Maximizing the benefits of Pilates-inspired exercise for learning functional motor skills. Journal of bodywork and Movement Therapies 4 (2): 99-108.
- Salbach M, Mayo NE, Higgins J, Ahmed S, Finch LE, et al. (2001) Responsiveness and predictability of gait speed and other disability measures in acute stroke. Arch Phys Med Rehabil 82(9): 1204-1212.
- Rossier P, Wade DT (2001) Validity and reliability comparison of 4 mobility measures in patients presenting with neurologic impairement. Arch Phys Med Rehabil 82(1): 9-13.
- Bohannon RW (1995) Sit-to-stand test for measuring performance of lower extremity muscles. Percept Mot Skills 80(1): 163-166.
- Newcomer KL, Krug HE, Mahowald ML (1993) Validity and reliability of the timed-stands test for patients with rheumatoid arthritis and other chronic diseases. J Rheumatol 20(1): 21-27.
- Kori SH, Miller RP, Todd DD (1990) Kinesiophobia: A new view of chronic pain behavior. Pain Management 35-43.
- Vlaeyen JW, Kole-Snijders AM, Rotteveel AM, Ruesink R, Heuts PH (1995) The role of fear of movement / (re)injury in pain disability. Journal of Occupationnal Rehabilitation 5(4): 235-252.
- French D, Roach P, Mayes S (2002) Fear of movement in injured workers: the Tampa scale of kiné Can J Behav Sci 34: 28-33.
- Leplège A, Ecosse E, Pouchot J, Coste J, Perneger T (2001) Le questionnaire MOS SF-36. Manuel de l'utilisateur et guide d'interprétation des scores. Editions Estem.
- Fox KH, Corbin CB (1989) The Physical Self-Perception Profile: Development and preliminary validation. Journal of sports et exercises psychology 11(4): 408-430.
- Ninot G, Delignières D, Fortes M (2000) L'évaluation de l'estime de soi dans le domaine corporel. Revue Staps 53: 35-48.
- Price DD, McGrath PA, Rafii A, Buckingam B (1983) The validation of visual analogue scales as a ratio scale for chronic and experimental pain. Pain 17(1): 45-56.
- Albazaz R, Wong YT, Homer-Vanniasinkam S (2008) Complex regional pain syndrome: a review. Ann Vasc Surg 22(2): 297-306.
- Henson P, Bruehl S (2010) Complex regional pain syndrome: state of the art update. Curr Treat Option Cardiovasc Med 12(2): 156-167.
- Ribbers GM, Geurts AC, Stam HJ, Milder T (2003) Pharmacologic treatment of complex regional pain syndrome I: a conceptual framework. Arch Phys Med Rehabil 84(1): 141-146.
- Lee HJ, Park HJ, Chae Y, Kim SY, Kim SN, et al. (2009) Tai Chi Qigong for the quality of life of patients with knee osteoarthritis: a pilot, randomized, waiting list controlled trial. Clinical Rehabilitation 23(6): 504-511.
- Wu G, Liu W, Hitt J, Millon D (2003) Spatial, temporal and muscle action patterns of Tai chi gait. Journal of electromyography and kinesiology 14(3): 343-354.
- Cruz-ferreira A, Fernandez J, Gomes D, Bernardo LM, Kirkcaldy BD, et al. (2011) Effects of pilates-based exercise on life satisfaction, physical self-concept and health status in adult women. Women & Health 51(3): 240-255.
- Goubert L, Crombez G, Van Damme S, Vlaeyen J, Bijttebier P, et al. (2004) Confirmatory factor analysis of the Tampa scale for kinesiophobia: invariant two-factor model across low back pain patients and fibromyalgia patients. Clinical Journal of Pain 20(2): 103-110.
- Roh S, Yoon S, Nyeon Kim J, Sung Lim H (2016) Effects of midified Pilates on variability of inter-joint coordination during walking in the elderly. J Phys Ther Sci 28(12): 3463-3467.
- Roelofs J, Sluiter JK, Frings-Dresen MH, Goossens M, Thibault P, et al. (2007) Fear of movement and (re)injury in chronic musculosketletal pain: Evidence for an invariant two-factor model of the Tampa Scale for kinésiophobie accros pain diagnoses and Dutch, Swedish, and Canadian samples. Pain 131(1-2): 181-190.
