 Case Report
Case ReportAbstract
Purpose: Peri-graft seroma (PGS) is defined as a sterile, serous fluid collection confined around a prosthetic vascular graft and rarely reported to be in pathophysiologic unknown cause.
Case Report: The authors experienced endovascular treatment of a peri-graft seroma that developed after open surgical repair of abdominal aortic aneurysm (AAA) with polytetrafluoroethylene (PTFE) graft. A 75-year-old man presented with growing aneurysm after open surgical repair of AAA with a PTFE bifurcated graft six years prior. The patient was referred to abdominal discomforts and physical exam revealed a palpable huge mass in the absence of tenderness, pulse, bruit and skin redness. Contrast enhanced computed tomography (CT) showed a huge peri-graft seroma measuring 112 mm in the longest diameter. The patient underwent endovascular PTFE graft relining with an Aortic extender, Excluder, and 10 mm x 10 cm stent-grafts, which named as Vaibhav. At 30 months follow-ups, CT revealed that a decreased seroma size from 112 mm to 59 mm in the longest diameter without flow disturbance.
Conclusion: Endovascular relining of the PTFE bifurcated graft should be considered as a treatment option for PGS of AAA.
Keywords: Endovascular Relining; EVAR; Peri-Graft Seroma; Abdominal Aortic Aneurysm
Abbreviations: AAA: Abdominal Aortic Aneurysm; CT: Computed Tomography; PTFE: polytetrafluoroethylene; PGS: Peri-Graft Seroma
Introduction
Peri-Graft Seroma (PGS) is a sterile, serous fluid collection confined around a prosthetic vascular graft in the original aneurysm sac [1-3]. Seromas are rarely reported after open repair of abdominal aortic aneurysm (AAA) [4-8]. Although the incidence of PGS after surgical treatment of AAA is rare, PGS compression by the seroma can cause variety of difficult problems, such as abdominal discomforts, infection, and graft thrombosis would be edams effect [9]. We report that PGS was that resolved with endovascular relining within open aortic repair polytetrafluoroethylene (PTFE) bifurcated graft (W. L. Gore & Associates) without open drainage of the seroma.
Case Report
A 75-year-old man presented with abdominal discomforts and a palpable mass without tenderness, pulse, and bruit. Six years prior to admission, the patient underwent open surgical repair of AAA with PTFE bifurcated graft (20 x 10 mm). The patient has a history of percutaneous coronary intervention 1 year prior and hypertension for 10 years. In admission lab revealed that there was no inflammation as normal range of WBC, ESR and CRP. Contrast enhanced computed tomography (CT) showed a huge peri-graft seroma measuring approximately 112 mm in the longest diameter. It began at the extend infrarenal aorta, extended to the middle of both iliac arteries, and was confined to the graft site. PET CT showed no evidence of infection in the seroma (Figure 1). Abdominal aortography showed no graft leakages or communication between the sac and arterial blood flow. The patient underwent endovascular relining of the PTFE bifurcated graft. A 23 mm Aortic Excluder (TM) extender (W.L. Gore & Associates, Inc., Flagstaff, AZ, USA) and 10 mm x 10 cm Vaibhans(TM) stent-grafts were used to reline the PTFE graft. The Excluder(TM) was deployed in the trunk of the PTFE graft. After relining the two aortic extenders, 10 mm x 10 cm Viabahns (TM) were successfully implanted within both iliac limbs. Ancillary attachment between original and new stent-grafts was made with a compliant balloon (Coda, Cookmedical Bloomington, IN, USA) and a 6 mm x 12 cm noncompliant balloon (Mustang, Boston Scientific, Marlborough, MA, USA) (Figure 2). Percutaneous aspiration was not performed for external drainage. A final aortogram was performed, and there was no evidence of endoleak or flow disturbance. At 6, 12, 24 months, and 30 months follow-ups, CT revealed no evidence of endoleak or flow disturbance and demonstrated decreased peri-graft seroma size of 76, 67, 61 mm and 59 mm gradually, respectively (Figure 3).
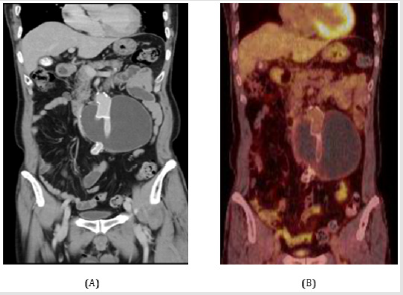
Figure 1:
A. CT scan shows large perigraft seroma and
B. PET scan shows no evidence of active infection at
first admission.
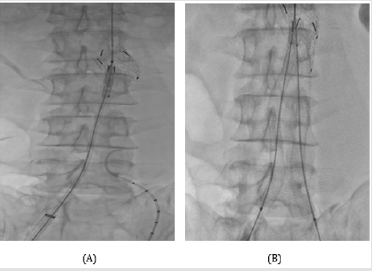
Figure 2:
A. One of the 23-mm Aortic extender was initially
deployed in the trunk of PTFE graft.
B. After the relining of another one, we two 10 mm - 10
cm sized stent-grafts were successfully implanted within
both iliac limbs with chimney technique.
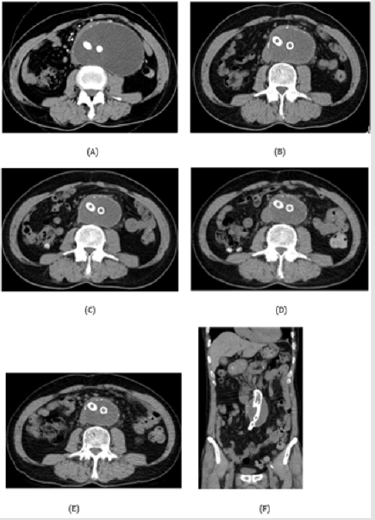
Figure 3: Follow-up CT scans reveal gradual regression of perigraft seroma at 0 (A), 6 (B), 12 (C), 24 (D) and 30 (E, F) months.
Discussion
PGS after open surgical repair of AAA is scarcely reported [4-8]. However, surgical procedures are not needed to resolve aymptomatic seromas [9,10]. If symptoms related to a seroma are present, such as abdominal discomforts, pain, ileus, or rupture, treatment of choice may require surgical methods till now [6,9,11]. However, PGS is difficult to diagnose during follow-up. In the early postoperative phase, it is hard to distinguish from postoperative fluid collections, such as hematoma, lymphocele, and infection. At the late postoperative phase, follow-up examinations such as CT scan and ultrasonography are usually selectively performed if a patient presents with any of symptoms or problems relation to the operation [12,13] In this case, CT was performed to ascertain the cause of symptoms reported by the patient who underwent surgical repair of AAA six years ago. It is also important to carefully screen patients with causative factors for PGS. Possible causative factors for PGS identified in the literature are as follows: failure of graft incorporation, insufficiency of graft fibrosis, and augmented graft permeability [1,3,4,6,9,14].
However, this case has no clear major causative factor for PGS. Although we can presume which causative factor is responsible for the development of PGS, there is no objective or effective tools for predicting failure of graft incorporation or insufficiency of graft fibrosis. It is possible that augmented graft permeability is related to excessive graft manipulation or pressurized irrigating solutions in the graft [9-14]. Therefore, this causative factor may be prevented by graft-controlled carefulness. PGS treatment options include percutaneous drainage of the aneurysm sac, open surgical drainage with an omental patch, surgical replacement of the PTFE graft with a Dacron (Intergard-WTM; Intra Vascular, Montvale NJ, USA) graft, and endovascular relining of the PTFE [1,3,5,6,9,15]. Of a variety of options, we selected endovascular relining of the PTFE as our first choice of therapy. Because the patient had a history of coronary heart disease, his cardiac load may have been adversely affected by open surgical methods. Open surgery would also be difficult to perform due to a history of laparotomy. We reasoned that an endovascular procedure would be safer to resolve the seroma. In this case, conventional EVAR was not indicated due to the short distance between the graft bifurcation and the lower renal artery (6 cm in length). The length of the aortic neck should be at least 7 cm, so a 23 mm Excluder (TM) and 10 mm x 10 cm Viabahn (TM) were used. There were no postoperative complications and no evidence of endoleak or flow disturbance. Decreased seroma size was observed at follow-ups of 6, 12, 24 months and 30 months. Although longterm surveillance is needed for endovascular treatment durability, endovascular relining is a good treatment option for PGS.
Conclusion
Endovascular relining of the PTFE bifurcated graft should be considered as a treatment option for PGS of AAA.
Conflicts of Interest
We declared no conflicts of interest at any potential financial and non-financial issues.
References
- Ahn SS, Machleder HI, Gupta R (1987) Perigraft seroma: clinical, histologic, and serologic correlates. Am J Surg 154(2): 173-178.
- Wolff T, Koller MT, Eugster T, Rouden C, Marti R, et al. (2011) Endarterectomy of the aneurysm sac in open abdominal aortic aneurysm repair reduces perigraft seroma and improves graft incorporation. World J Surg 35(4): 905-910.
- Blumenberg RM, Gelfand ML, Dale WA (1985) Perigraft seromas complicating arterial grafts. Surgery 97(2): 194-204.
- Williams GM (1998) The management of massive ultrafiltration distending the aneurysm sac after abdominal aortic aneurysm repair with a polytetrafluoroethylene aortobiiliac graft. J Vasc Surg 28(3): 551-555.
- Risberg B, Delle M, Eriksson E, Klingenstierna H, Lönn L, et al. (2001) Aneurysm sac hygroma: A cause of endotension. J Endovasc Ther 8(5): 447-453.
- Thoo CH, Bourke BM, May J (2004) Symptomatic sac enlargement and rupture due to seroma after open abdominal aortic aneurysm repair with polytetrafluoroethylene graft: implications for endovascular repair and endotension. J Vasc Surg 40(6): 1089-1094.
- Lucas LA, Rodriguez JA, Olsen DM (2009) Symptomatic seroma after open abdominal aortic aneurysm repair. Ann Vasc Surg 23(2): 144-146.
- Cuff RF, Thomas JH (2005) Recurrent symptomatic aortic sac seroma after open abdominal aortic aneurysm repair. J Vasc Surg 41(6): 1058-1060.
- Ajith K Kadakol, Timothy J, Lin JC, Weaver MR, Karam JL, et al. (2011) Frequency risk factors and management of perigraft seroma after open abdominal aortic aneurysm repair. J Vasc Surg 54(3): 637-643.
- Sangawa K, Aoki A (2013) Endovascular treatment of perigraft seroma after open abdominal aortic aneurysm repair: Report of a case. Ann Vasc Dis 6(2): 218-220.
- Stierli P, Gurke L, Hess P, Th Eugster, F Harder, et al. (2000) Aneurysm sac enlargement after conventional inflammatory aneurysm repair with a polytetrafluoroethylene aortobiiliac graft. Eur J Vasc Endovasc Surg 20(5): 484-486.
- Akiyama K, Takazawa A, Hirota J, Yamanishi H, Akazawa T, et al. (1999) Bleeding through the fiber interstices of a knitted Dacron graft 12 years after its implantation: report of a case. Surg Today 29(9): 953-956.
- Stierli P, Gurke L, Hess P, Th Eugster, F Harderet, et al. (2000) Aneurysm sac enlargement after conventional inflammatory aneurysm repair with a polytetrafluoroethylene aortobiiliac graft. Eur J Vasc Endovasc Surg 20(5): 484-486.
- Salameh MK, Hoballah JJ (2008) Successful endovascular treatment of aneurysm sac hygroma after open abdominal aortic aneurysm replacement: a report of two cases. J Vasc Surg 48(2): 457-460.
- Sangawa K, Aoki A (2013) Endovascular treatment of perigraft seroma after open abdominal aortic aneurysm repair: report of a case. Ann Vasc Dis 6(2): 218-220.
