 Short Communication
Short CommunicationIntroduction
Heart diseases become one the main civilization diseases also in Poland. As consequence, coronary angiography (CORO) with following percutaneous coronary intervention (PCI) is the most frequently performed interventional procedure in cardiology with more than 200.000 procedures performed yearly in Poland (2013) [1]. Level of radiation risk in IC procedures is highly dependent on the clinical condition and physiology of patient but also on the technical quality of imaging equipment (i.e. angiographs). The aim of this paper was to evaluate a significance of technological solutions in angiographs used for coronary angiography with following percutaneous coronary intervention (CORO+PCI) for radiation risk to adult patients.
Methods
X-ray doses obtained in CORO+PCI procedures performed under control of three angiographs currently offered by main producers, i.e.: Allura Clarity (made by Philips), Artis Zee (made by Siemens) and Infinix X (made by Canon-previeously Toshiba) were compared. The doses were evaluated experimentally using thermoluminescent (TL) dosemeters made by Ladis Laboratory (Krakow, Poland). Patient during exposure was imitating by the physical antropomorphic phantom (CIRS, USA) representing standard-size adult man. All the exposures were performed in a routine fashion, according to the same “standardized” working schedule being elaborated on the basis of direct careful observation of real patients’ treatment.
Exposure conditions for all dosimetrically evaluated procedure
were as follows:
1. Radiography: 2 times at about 80 kV (mAs -set
automatically) at LAO-200 and SID=100 cm,
2. CORO- pulsed fluoroscopy:
a) RAO 20/CAUD 30: 20 s,
b) LAO 40/CAUD 2: 18 s,
c) LAO 4/CRAN 37: 21 s,
d) LAO 30/CAUD 40: 22 s;
3. PCI - Pulsed fluoroscopy LAO 40/CAUD 20: 9.5 minutes;
4. Acquisition (fluorography) : 5-6 s projections according
CORO-2(a, b, c, d) and 20 s according PCI -
Results
The results of measurements performed at above parameters
are presented in Table where the following values are given:
a) Doses absorbed in the organs situated in body volume
cover by primary X-ray beam,
b) Effective dose and
c) Air karma in the reference point.
(The last quantity is measured automatically by angiographic
system and displayed on the monitors.)
The effective doses (as a measure of future health effects
probability) were also computed according ICRP recommendations
[2-3] (Table 1).
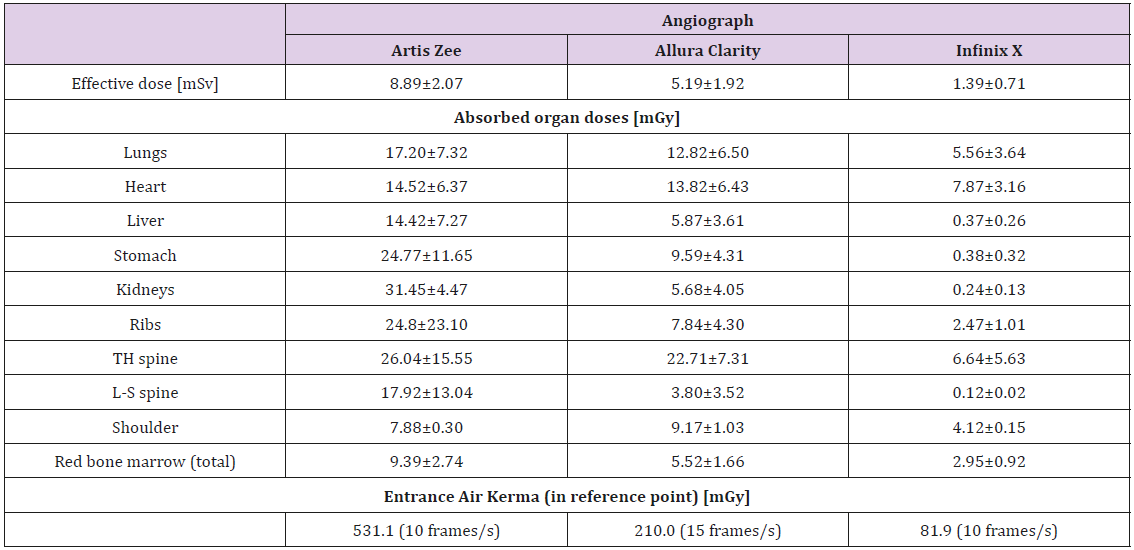
Table 1: Absorbed doses (in mGy) and effective dose (in mSv) for adult patient and air kerma (in mGy).
The obtained results were statistically analyzed using nonparametric
Wilcoxon’ test sum of rank (in wider version Mann-
Whitney-Wilcoxon). The statistical probe was completed from dose
values obtained during exposure performed the given angiograph.
The compared probes were independent and had the same number
of elements. Value of test statistic (W) was calculated as sum of
ranks and critical value at assumed significance level was checked
in the appropriate statistical tables [4]. As the result, the following
relationships among the dose values for adult patients in CORO+PCI
procedures under control of compared angiographs were found:
1) Artis Zee - Allura Clarity : differ at significance level α =
0.02,
2) Artis Zee - Infinix : differ at significance level α = 0.02,
3) Allura Clarity - Infinix : differ at significance level α = 0.02,
It should be underlined that the dose differences were found
despite:
1. The same “patient” (i.e. antropomorphic phantom),
2. The same angles of projections, time of X-ray emission
and distance to focus of X-ray tube.
Discussion and Conclusions
The observed differences can be explained by a diverse action of automatic exposure control (AEC) for the compared angiographs resulting in different dynamics of dose increasing. Additionallyan automatic change of filtration in dependence on thickness of examined object (patient) is implemented in Artis Zee and Infinix. As consequence, when a part of the spine or the ribs are covered by primary X-ray beam the intensity and penetrability of radiation becomes higher and doses for deep organs placed on directory of primary beam are also higher.
Because of that, for angiographs with such high dynamics of AEC system better quality of images for big-size patients is easier to obtain, although the angles of particular projections should be set very carefully. Size of primary beam area is also important for dose level.
Characteristic feature of exposure in interventional radiology procedures is the possibility of high irradiation of relatively small areas of patient’ body (dependently on procedure type). For IC procedures this problem concerns of course the whole heart, but also part of the lung (mainly right one), part of TH-spine and the ribs. The dose for these parts can be really high, even if average absorbed doses for the organs /body parts are quite acceptable and organ remain undamaged. Taking this into consideration the selection of angiograph and knowledge its functioning is crucial for safe usage the device by medical teams.
References
- Ochala A, Legutko J, Siudak Z, Parma R, Chmielak Z, et al. (2014) Statistics regarding interventional cardiology in Poland in 2013. Summary report of the Association of Cardiovascular Interventions of the Polish Cardiac Society (AISN PTK). Kardiologia Polska 72(12): 1402-1407.
- Cornetto AP, Aimonetto S, Pisano F, Guidice M, Sicuro M, et al. (2016) The contribution of interventional cardiology procedures to the population radiation dose in a “health-care level I” representative region. Radiation Protection Dosimetry 168(2): 261-270.
- (2007) The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann ICRP 37(2-4): 1-332.
- R Zieliński (1972) Statistical tables. PWN, Warsaw 1972, tabl 53 pp. 300- 303.
