 Research Article
Research ArticleAbstract
Introduction: This study was made to evaluate the effect of the use of endoscopic probe and orogastric tube for the guidance of gastric resection line, on early term results and peroperative and postoperative complications of the bariatric procedure.
Methods: A retrospective study was performed at the Education and Research Hospital of Van (Van, Turkey) between January 2015 and December 2017. Laparoscopic sleeve gastrectomy was performed on both groups (group 1: orogastric tube calibration group, group 2: endoscopic probe calibration group). The calibration technique was chosen by the availability of the endoscopist at the time of the surgery. Surgery and endoscopy were performed by the same medical team.
Results: Eighty-five patients undergoing laparoscopic sleeve gastrectomy were randomly allocated to two groups. 62 females (73%) and 23 males (27%) with a manage of 37.9 years and a preoperative mean body mass index of 45.5 kg/m². In the both two groups no bleeding point on the gastric resection line was detected. There were no significant differences in the operation time, calibration time, demographic data’s and BMI between two groups. It is easier to make the calibration by the orogastric tube because the number manipulation is dramatically less for the calibration. But the use of the gastroscope probe for the calibration of the gastric sleeve, instead of the Standard use of the bougie or the orogastric tube; is a safe procedure and the surgeon has a higher sense of security and a higher amount of visuality.
Conclusion: There were no significant differences in preoperative and postoperative complications between two calibration groups although a larger study is required to reach a definitive conclusion.
Keywords: Sleeve Gastrectomy, Orogastric Tube, Bariatric Surgery
Introduction
Laparoscopic surgical procedures have become increasingly popular in recent years. The reasons such as less surgical stress and faster recovery are the main reasons for this increase in popularity [1]. Laparoscopic sleeve gastrectomy is one of the most frequently used bariatric surgery procedures in the surgical treatment of morbid obesity. In addition, advances in laparoscopic surgery, also there have been serious developments in bariatric surgery and current surgical approaches [2]. It is necessary to increase use of materials that provides shortening of operation time, reducing perioperative complications and facilitating the operation technically. Orogastric tubes and endoscopy probes are the instruments which are used as a guide in determining the resection line in the preparation of gastric residue pouch in laparoscopic vertical sleeve gastrectomy procedure. The preparation of the gastric pouch is an important step of the operation, so the tools used in the preparation of this pouch are also important. In our randomized, comparative, retrospective study, we aimed to evaluate the orogastric tube and endoscopy probe which are used for these purposes, mentioned in terms of advantages and disadvantages.
Materials and Methods
On the bariatric surgery topic, the fact that such studies have been performed less frequently is the most important factor in determining the power analysis of the study in terms of sample size. Between January 2015 and December 2017; A total of 85 patients with body mass index greater than 40 or with a body mass index greater than 35 and with at least one comorbid disease were included in the study randomly. Patients with esophagus or stomach disease, who have a history of previous operations, patients who were evaluated as difficult intubation after anesthesia consultation were excluded from the study. The surgeons and the surgical team participated in more than 50 operations using both the orogastric tube and the gastroscope probe before the evaluations began. All operations were performed by the same surgical team. In this study, Visigi 3D® 40 Fr. Tube was used as orogastric probe and Fujinon EG600® 36 Fr. as the gastroscope probe. Standard laparoscopic vertical sleeve gastrectomy procedure was performed in both groups. The orogastric tube in 43 patients in group 1, and the gastroscopy probe in 42 patients in group 2 were used for calibration determining of gastric resection line. Age, gender, height, weight and body mass index of the patients were recorded. The time of placement of the calibration equipment which is used for the determination of the gastric resection line, the total operation time, and the amount of bleeding in the gastric resection line were carefully monitored and recorded. Materials used to calibrate the gastric resection line were performed when patients were in Trendelenburg position. While the surgeon who did not join the operation advanced the gastroscope probe, the orogastric tube was advanced by the anesthetist along the small curvature of the stomach. The basis of our study; The measurement of the insertion times of the instruments used for the stomach calibration into the esophagus from the mouth to the stomach and finally to the distal part of the pylorus. The measurements were started with advancing of the calibration tube or probe from mouth to the esophagus by the anesthetist or endoscopist and finished with instrument’s passing the vehicle from the pylorus to the duodenum. In all operations; before the insertion of calibration instrument into the stomach, the stomach lumen was evacuated by using a nasogastric catheter and the stomach was done completely empty. The manipulation and maneuver numbers which were done for positioning of calibration instrument were also recorded. Orogastric tube or gastroscope probe was passed through the pylorus and inserted duodenum by the surgeon visually. The amount of bleeding in the resection line is; calculated by measuring the amount of blood aspirated from the intra-abdominal cavity.
Statistical Analysis
Statistical analysis; The ready-to-use statistics program for Windows10® was made using SPSS® version 19. Data were analyzed using student t test (Mann Whitney U test and chi-square test used for comparison of qualitative values). P values less than 0.05 were considered statistically significant.
Results
Results from 85 patients included in the study were analyzed. Group 1; 43 patients with orogastric tube, group 2; that is, 42 patients with gastroscopy probe were randomized. Forty-three patients with orogastric tube were randomized as Group 1, 42 patients with gastroscopy probe were randomized as Group 2. Among the groups; There was no significant difference in terms of age, gender, height, weight and body mass index (Table 1).

Table 1: Distribution of demographic data and BMI by groups.
When intraoperative data are evaluated; Positioning times to the calibration device, in orogastric tube inserted group; 7.5 ± 2 min,9 ± 1.5 minutes in the group using gastroscopy probe; and was similar in both groups (p = 0.15). In terms of total operation time, group 1 was recorded as 55.1 ± 12.3 min and in group 2 as 61.5 ± 15 min. Although there was no statistically significant difference between the groups (p = 0.06), the total operation time was shorter in cases with orogastric tube group 1. The bleeding levels were 110 ± 195 mL in the orogastric tube group and 102.5 ± 70 mL in the gastroscopy probe group were recorded and they were similar in both groups (p = 0.81) (Table 2).
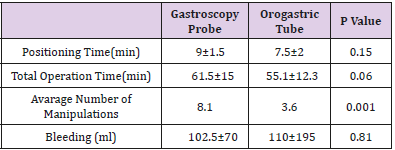
Table 2: Comparison of the groups for durations, manipulation numbers and bleeding amounts.
The number of manipulations to the calibration equipment was also recorded. The average number of manipulations for positioning orogastric tube in duodenum recorded 3.6, and the number of using FUJINON® gastroscope probe for same insertion was 8.1. It was determined that the number of manipulations for placing the orogastric tube in the correct position was significantly less and more comfortable position could be given (p = 0.001) (Figure 1).
Figure 1: Number of manipulations by groups.
Discussion
According to many surgeons; When applying laparoscopic sleeve gastrectomy procedure, it is important to note that the gastric volume should not be too narrowed while the stomach volume should be reduced sufficiently [3]. This is because at the beginning of the most frequently observed complications are clinically symptomatic strictures (1%) in the six-week postoperative period [4]. The incisura angularis area has the highest potential for stenosis in the stomach lumen [5]. The lateral symmetrical traction of this region prevents 75% constriction, whereas the development of stenosis after resection with a calibration tool of the same area can be prevented by 82% [5]. The most effective treatment after stenosis is considered to be roux-y gastric bypass [4]. Villalonga and colleagues confirmed that both the endoscopy probe and the VISIGI 3D® orogastric tube were able to aspirate the lumen of the stomach and allow lateral traction to be more comfortable as similar as the present study. Thus, it was concluded that the incidence of dysphagia and related malnutrition decreased significantly in the postoperative period [4]. In 2008, Frezza et al. Performed an endoscopic guided laparoscopic vertical sleeve gastrectomy procedure in 20 patients and completed this procedure without any complication [6]. A similar study was carried out by Kockerling and Schug Pass in 38 patients in 2010 and achieved almost the same results as the Frezzan [7]. Because of the fact that the endoscopy probe can be manipulated in all directions from the calibration tools used, we have seen that the orogastric tube has a statistically significant advantage in terms of the number of manipulations in positioning. Because the orogastric tube did not lose its position easily once after passing the pylorus due to the inclination of the small curvature anatomy of the stomach. However, when the total calibration times and operating times are examined; The difference between group 1 and group 2 was not statistically significant.
One of the most feared complications that may occur during calibration is laparoscopic sleeve gastrectomy; iatrogenic perforations that may occur in the lumen of the stomach or esophagus [8]. In our study, no perforation occurred in both groups. The distal portion of the VISIGI 3D® orogastric tube is made softer to reduce the risk of perforation. The gastroscopy probe has a much more rigid structure. Therefore, the potential of the orogastric tube to cause perforation is thought to be much lower [8]. A perforation, especially in the esophagus, can lead to mediastinitis and so lifethreatening clinical conditions [9]. In addition, in the resection section of the laparoscopic sleeve gastrectomy procedure, the spark plug, intraluminal heat probes and orogastric tubes can be transected with the stapler device. Many cases are mentioned in the literature regarding this complication [10]. There is no possibility of transecting the endoscope probe with stapler. Accidental transection of these tubes significantly increases morbidity, mortality and operation time [10]. Regarding to this complication, Dr. Üstün posted a masterful video. Repair of the transected gastric wall with primary sutures and repair of technical facilities with robotic surgery are recommended by him [11].
Conclusion
As a result of our study we have seen; One of the effective surgical methods of morbid obesity is laparoscopic vertical sleeve gastrectomy. Both orogastric tubes and endoscopy probes used for calibration in the gastric pouch preparation phase in the laparoscopic sleeve gastrectomy procedure are shorten the operation time. While there was no significant difference between the application times of these 2 calibration tools, we found that the orogastric tube could be placed more easily by requiring less manipulation due to its structure. However, we believe that the endoscopy probe is safer than orogastric tube because of having no possibility of transection. And we think that these 2 calibration tools can be used effectively in these procedures.
Conflict of Interest
All authors read and approved the final manuscript. Also, the authors declare that they have no conflicts of interest.

Comparison of Orogastric Tube and Endoscopy Probe in the Laparoscopic Vertical Sleeve Gastrectomy Operations
Abstract
Introduction: This study was made to evaluate the effect of the use of endoscopic probe and orogastric tube for the guidance of gastric resection line, on early term results and peroperative and postoperative complications of the bariatric procedure.
Methods: A retrospective study was performed at the Education and Research Hospital of Van (Van, Turkey) between January 2015 and December 2017. Laparoscopic sleeve gastrectomy was performed on both groups (group 1: orogastric tube calibration group, group 2: endoscopic probe calibration group). The calibration technique was chosen by the availability of the endoscopist at the time of the surgery. Surgery and endoscopy were performed by the same medical team.
Results: Eighty-five patients undergoing laparoscopic sleeve gastrectomy were randomly allocated to two groups. 62 females (73%) and 23 males (27%) with a manage of 37.9 years and a preoperative mean body mass index of 45.5 kg/m². In the both two groups no bleeding point on the gastric resection line was detected. There were no significant differences in the operation time, calibration time, demographic data’s and BMI between two groups. It is easier to make the calibration by the orogastric tube because the number manipulation is dramatically less for the calibration. But the use of the gastroscope probe for the calibration of the gastric sleeve, instead of the Standard use of the bougie or the orogastric tube; is a safe procedure and the surgeon has a higher sense of security and a higher amount of visuality.
Conclusion: There were no significant differences in preoperative and postoperative complications between two calibration groups although a larger study is required to reach a definitive conclusion.
Keywords: Sleeve Gastrectomy, Orogastric Tube, Bariatric Surgery