 Case Report
Case ReportAbstract
Cardiac stress testing, using treadmill exercise, is the basic screening tool for the early detection of Coronary Artery Disease (CAD). Patients with positive stress testing usually undergo a Myocardial Perfusion Imaging (MPI) study. The demonstration of abnormal blood flow distribution, indicative of functionally significant myocardial ischemia, leads to the performance of coronary angiography. Angiographic investigation is considered as the current gold standard method in CAD diagnosis, and generally provides the required information to the clinicians for the proper management of the patients. Nevertheless, despite MPI evidence of ischemia, coronary angiography does not reveal abnormal coronary arteries in a significant number of patients. We present a case of a male patient with positive treadmill exercise and MPI findings but no angiographic evidence of CAD. Further, we discuss the implications for the proper management of patients with the above mentioned combination of findings after extensive work-up.
Keywords: Coronary Artery Disease; Coronary Angiography; Myocardial Perfusion Imaging; Myocardial Ischemia
Introduction
A diagnostic and therapeutic dilemma is often posed in patients with evidence of functional ischemia based on Myocardial Perfusion Imaging (MPI), but negative subsequent coronary angiography results. Although these MPI studies are often dismissed as ‘’falsepositive’’, complete agreement between scintigraphic imaging and angiographic findings should not be expected, since coronary angiography provides anatomical information, while MPI evaluates the hemodynamic consequences of several parameters, including endothelial function, small vessel function, and collateralization [1]. We present a case of a male patient with positive treadmill exercise and MPI findings but no angiographic evidence of Coronary Artery Disease (CAD).
Case Report
A male patient, 50 years old, was referred to the Department of Nuclear Medicine, Army Share Fund Hospital (417 NIMTS), for a clinically indicated MPI. One-day stress/rest MPI was performed using technetium-99m (99mTc) sestamibi (Cardioscan, National Centre for Nuclear Research, Otwock, Poland), following cardiac stress according to the Bruce protocol. Due to anginalike chest pain, the patient had undergone treadmill test, which was positive. Rest echocardiography was normal, with ejection fraction 60%. During the exercise component of the study, the recorded electrocardiographic changes were also suggestive of myocardial ischemia. Scintigraphic imaging revealed the presence of moderate ischemia at part of the inferior wall and a small part of the posterolateral wall of the left ventricle (Figure 1a). Based on the stress electrocardiographic and scintigraphic findings, coronary angiography was performed, which was completely normal (Figure 1b).
Discussion
Cardiac syndrome X represents an ambiguous area of the coronary disease spectrum, in which patients show anginalike chest pain combined with either normal or abnormal MPI. Commonly, despite extensive work-up, no cardiac or non-cardiac causes can be revealed for the observed clinical features in these patients who continue to suffer from angina-like chest pain. In particular, no intraluminal lesions or <50% narrowing of one or more coronary arteries are demonstrated in about 48% of females and 17% of males undergoing coronary angiography annually [2].
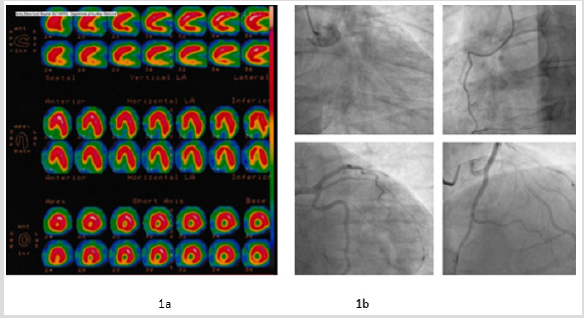
Figure 1: One-day stress/rest myocardial perfusion imaging revealed moderate ischemia at parts of the inferior and posterolateral walls of the left ventricle (Figure 1a). Despite positive stress electrocardiographic and scintigraphic findings, coronary angiography was normal (Figure 1b).
Jonson et al. proposed that the underlying pathophysiology of myocardial ischemia in females without CAD diagnosis should be further investigated, given the higher rate of angina-related hospitalizations, repeat catheterization, and greater treatment costs [3]. Based on the available data, cardiac syndrome X is more commonly observed in middle-aged Caucasian females, who may have additional characteristics, such as a strong CAD family history and pro-thrombotic states [4]. Initially, it was not associated with increased risk of future cardiac events [5]. However, the risk of cardiac events was found to be increased when the syndrome co-existed with endothelial dysfunction [6,7]. Interestingly, the microvascular origin of the syndrome is supported by its associations with features of the metabolic syndrome and migraine headache disease [8].
Although cardiac syndrome X had been exclusively related to female sex, more recent research concluded that >43% of patients, meeting the criteria of the syndrome, are males [9]. In a malepredominant cohort of chest pain patients, Addison et al. found that the demonstration of ischemia on MPI was linked to higher long-term risk of adverse cardiac events despite subsequent negative coronary angiography, in comparison to those with no MPI-confirmed ischemia [10]. Similarly, in older male veterans, Delcour et al. reported a higher prevalence of cardiovascular events associated with abnormal MPI findings [11].
Conclusion
The long-term risk of adverse events in patients with cardiac syndrome X remains controversial and can pose crucial dilemmas for clinicians in terms of proper management and follow-up. The use of calcium channel-blockers coupled with anti-platelet therapy has been suggested [10]. Moreover, treatment options improving endothelial function, such as angiotensin-converting enzyme inhibitors, statins and lifestyle modifications, may be of value [10]. Finally, further changes in myocardial blood flow distribution could be also detected through the performance of cardiac imaging studies.
Conflict of Interest
All authors declare no conflict of interest
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
- Angelidis G, Samara M, Papathanassiou M, Satra M, Valotassiou V, et al. (2018) Impact of renin-angiotensin-aldosterone system polymorphisms on myocardial perfusion: Correlations with myocardial single photon emission computed tomography-derived parameters. J Nucl Cardiol 26(4): 1298-1308.
- Pepine CJ, Balaban RS, Bonow RO, Diamond GA, Johnson BD, et al. (2004) Women's Ischemic Syndrome Evaluation: current status and future research directions: report of the National Heart, Lung and Blood Institute workshop: October 2-4, 2002: Section 1: Diagnosis of stable ischemia and ischemic heart disease. Circulation 109(6): e44-e46.
- Johnson BD, Shaw LJ, Buchthal SD, Merz CN B, Kim HW, et al. (2004) Prognosis in women with myocardial ischemia in the absence of obstructive coronary disease: Results from the national institutes of health-national heart, Lung, and blood institute-sponsored Women's Ischemia Syndrome Evaluation (WISE). Circulation 109(24): 2993-2999.
- Cannon RO (2009) Microvascular angina and the continuing dilemma of chest pain with normal coronary angiograms. J Am Coll Cardiol 54(10): 877-885.
- Hurst T, Olson TH, Olson LE, Appleton CP (2006) Cardiac syndrome X and endothelial dysfunction: new concepts in prognosis and treatment. Am J Med 119(7): 560-566.
- Mering GO V, Arant CB, Wessel TR, McGorray SP, Merz CN B, et al. (2004) Abnormal coronary vasomotion as a prognostic indicator of cardiovascular events in women: Results from the national heart, lung, and blood institute-sponsored Women's Ischemia Syndrome Evaluation (WISE). Circulation 109(6): 722-725.
- Halcox JP, Schenke WH, Zalos G, Mincemoyer R, Prasad A, et al. (2002) Prognostic value of coronary vascular endothelial dysfunction. Circulation 106(6): 653-658.
- Wessel TR, Arant CB, McGorray SP, Sharaf BL, Reis SE, et al. (2007) Coronary microvascular reactivity is only partially predicted by atherosclerosis risk factors or coronary artery disease in women evaluated for suspected ischemia: Results from the NHLBI Women's Ischemia Syndrome Evaluation (WISE). Clin Cardiol 30(2): 69-74.
- Vermeltfoort IA, Raijmakers PG, Riphagen II, Odekerken DA, Kuijper AF, et al. (2010) Definitions and incidence of cardiac syndrome X: Review and analysis of clinical data. Clin Res Cardiol 99(8): 475-481.
- Addison D, Singh V, Asante KO, Okafor H (2014) Cardiovascular outcomes of a positive nuclear stress test but negative coronary angiography in a multiethnic male predominant cohort. Niger Med J 55(1): 14-19.
- Delcour KS, Khaja A, Chockalingam A, Kuppuswamy S, Dresser T (2009) Outcomes in patients with abnormal myocardial perfusion imaging and normal coronary angiogram. Angiology 60(3): 318-321.
