 Research Article
Research ArticleAbstract
Background: Congenital Cytomegalovirus infection is the main non-genetic cause of hearing loss in infants. The immune assay enzyme is used to detect the specific immunoglobulin M Cytomegalovirus. The Auditory Brainstem Response (ABR) is used to detect the V wave.
Objective: To determine the relationship between the dB of the V wave and Cytomegalovirus specific immunoglobulin M (IgM) levels in patients with congenital Cytomegalovirus infection.
Methods: This study used a cross-sectional design at Dr. Sardjito General Hospital,
Yogyakarta, between early January 2014 until the end of December 2018. The inclusion
criteria were;
a) Child patients with a diagnosis of congenital Cytomegalovirus infection
b) Performed ABR, and
c) Performed Cytomegalovirus specific immunoglobulin tests. The exclusion criteria
were the subjects who refused to participate in this research. All subjects underwent
examination for IgM levels and detection of the appearance of V waves. Total sample size
was 47 subjects.
Results: There were 16 (34%) female and 31 (66%) male research subjects who participated in this research. The average V wave detected in the right ear was 73.7234 ± 28.46562 dB, while the left ear was 71.80851 ± 27.78852 dB, which was not statistically significant. The average IgM CMV titer for all samples was 0.282553 ± 0.068832 IU/ mL. Correlation coefficient between right and left ear with IgM level was 0.57 and 0.58, respectively.
Conclusion: It can be concluded that there is a strong correlation between dB V wave appearance from ABR examination with Cytomegalovirus-specific levels of immunoglobulin M (IgM) in patients with congenital Cytomegalovirus infection.
Keywords: Cytomegalovirus Specific Immunoglobulin M (IgM) Levels; Db Emergence Wave V; Relationship; Congenital Cytomegalovirus Infection; Infant
Abbreviations: ABR: Auditory Brainstem Response, IgM: Cytomegalovirus Specific Immunoglobulin M, CMV: Cytomegalovirus, SNHL: Sensorineural Hearing Loss, OAE: Otoacoustic Emission, MHREC: Medical and Health Research Ethics Committee
Introduction
Cytomegalovirus (CMV) infection in humans usually involves a complex balance between viruses and hosts, which results in persistent and dormant infections. CMV in humans encodes various types of protein genes that can affect the activation of host cells, leukocytes, inflammatory responses, as well as active and passive immunity defenses that causes persistent infection of CMV in the human body [1]. Women with primary CMV infection during pregnancy have a greater risk of giving birth to children with congenital CMV infection, which has an incidence of around 40%. Autopsy studies of fetuses and newborns with congenital infections show that CMV infects various types of cells and causes damage to organs, including defects in the cochlea, vestibular, and auditory canal causing hearing loss in infants [2]. Some population-based research in Sweden, America and Canada reported that between 9.3-17% of newborns with congenital CMV (cCMV) infection will suffer from sensorineural hearing loss (SNHL). The incidence of SNHL is 22-41% in infants with clinical symptoms, and 6-16% in infants who are asymptomatic or have subclinical symptoms [2,3]. The Immune assay enzyme is often used to detect IgG and IgM CMV. IgG serum can be used to determine the history of previous CMV infections, namely for knowing the risk of viral (blood and organ donor) transmission, and the risk of reactivation in immunocompromised patients. IgM serum is used to determine the presence of primary infection in patients [4]. Otoacoustic Emission (OAE) procedure is an examination option that can be done for the purpose of screening cochlear function. The Auditory Brainstem Response (ABR) can be tested as an auditory nerve function test [5]. This study aimed to determine the relationship between the dB emergence of the V wave in the ABR examination results and Cytomegalovirus specific immunoglobulin M (IgM) levels in patients with congenital Cytomegalovirus infection.
Methods
This study used a cross-sectional study design. The study was
conducted at the Otorhinolaryngology Department and Pediatric
Department Faculty of Medicine Universitas Gadjah Mada/ Dr. Sardjito
General Hospital Yogyakarta from early January 2014 until the
end of December 2018. The study started after receiving approval
from the Medical and Health Research Ethics Committee (MHREC)
Faculty of Medicine, Public Health and Nursing, Universitas Gadjah
Mada, Yogyakarta, Indonesia under number KE/FK/0352/
EC/2019. The research subjects of this study were all patients with
a diagnosis of congenital cytomegalovirus infection (cCMV). Sample
size was calculated using a hospital-based study sample size formulation
for cross-sectional study with error type I (α) 5% one-tailed
hypothesis, and error type II (β) 20%. The recommended sample
size was 47 samples. Characteristics data of research subjects are
presented as proportion, mean, standard deviation and correlation.
The study began by identifying the cCMV infected groups and then
comparing immunoglobulin M levels and the dB emergence of the V
wave in the results of the ABR examination. Inclusion criteria were:
a) Child patients with a diagnosis of congenital Cytomegalovirus
infection
b) Performed ABR examination, and
c) Performed Cytomegalovirus specific immunoglobulin
tests. The exclusion criteria were parents of the subjects who
refused to participate in this research. The minimum number
of samples was 47 samples of patients with cCMV infection.
Results
Table 1 shows there were 16 (34%) female and 31 (66%) male research subjects who participated in this research. Based on the dB emergence of the V wave in results of the ABR examination in right ear, the average was 73.7234 ± 28.46562 dB, while in left ear it was 71.80851 ± 27.78852 dB, which was not statistically significant. The average IgM CMV titre for all samples was 0.282553 ± 0.068832 IU/mL. From all 47 subjects, 39 (82.96 %) subjects were determined as symmetrical abnormal, and 8 (17.04 %) were asymmetric abnormal.
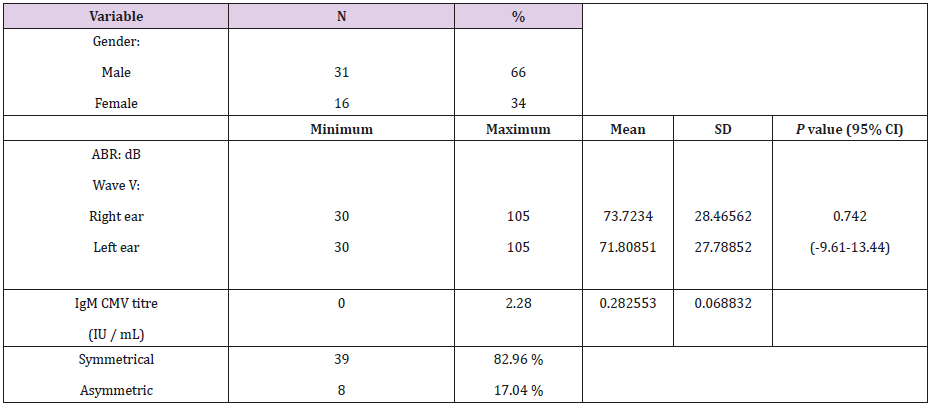
Table 1: Characteristics of research subjects.
Discussion
The sex of the subject in this present study was 31 (66%) male subjects, and 16 (34%) female subjects. There were considerably more male subjects than female subjects, with almost 2:1 ratio. Other studies showed no statistically significant differences in the incidence of congenital Cytomegalovirus infection by sex [6]. Immunoglobulin M examination conducted in this study sample obtained 5 patients with positive results (9.6%), namely with titres ≥0.70 IU / mL, and 47 (90.4%) patients who were negative with titres <0.70 IU/mL. With increasing age, the tendency of IgM production will decrease, and IgG production can be stable or increase depending on the patient’s own condition. The results of a low IgM titre examination alone cannot be attributed to the absence of congenital cytomegalovirus infection in patients, and conversely diagnosis is difficult to establish if IgM is not detected in serum [2,7]. In this present study, left and right ear hearing loss was found in 39 (84.6%) subjects suffering from symmetrical hearing loss in both ears, while 8 (15.4%) suffered from asymmetrical hearing loss. Mizuno et al. (2009) stated that asymmetrical hearing loss is often found in children with cCMV infection, with various proportions [8]. Another study found that as many as 38% of children with cCMV infection suffered from asymmetrical hearing loss. One study with a mouse model found there were varied losses ranging from 40% to 46% [9]. This asymmetrical hearing loss can be caused by the dissemination of the meningogenic virus from the central nervous system to the inner ear at different rates, as well as the asymmetrical immune response of the two cochleae [8,10,11].
A targeted CMV approach that tests newborns who fail their newborn hearing screening (NHS) can identify the majority of infants with CMV-related neonate NHS at birth. However, 43% of the infants with CMV related sensorineural hearing loss (SNHL) in the neonatal period and cCMV infants who are at risk for late onset SNHL who were not identified by NHS [12] Congenital CMV (cCMV) infection is the main non-genetic cause of sensorineural hearing loss, implicated in 0.5 per 1000 births, or 8% of cases of hearing loss and taking into an account all levels of severity together, it is estimated to be responsible for 20% of cases of hearing loss of unknown origin. Hearing loss secondary to cCMV infection is not caused by direct sensorineural involvement but rather impairment of the homeostasis regulation structures of the inner ear [13]. Some research was unable to define the timing of virus transmission to the fetus which limits any definitive interpretation of these studies. The literature suggests that the role of viral load measurements in predicting CMV-associated SNHL is unclear at the present time [14]. Intrauterine CMV transmission may occur in mothers without preexisting immunity who first acquire CMV infection in pregnancy (primary infection), or in women with preexisting antibodies to CMV either by reactivation of a previous maternal infection or by acquisition of a different viral strain (non-primary infection). Primary CMV infections are associated with the greatest risk of in-utero transmission with incidence ranging from 30–35%, while for non-primary infections the transmission rate is significantly lower at 1.1–1.7% [15]. There is no pathognomonic configuration of hearing loss caused by cCMV. Rather, it is characterized by its unstable nature, with rapid progression and fluctuations [16]. One study reported that an additional 900 infants with asymptomatic cCMV infection are estimated to have SNHL within 8 weeks of life, although nearly half of these infants are likely missed by NHS [17].
In this present study, the correlation coefficient (r) that was found in the result of the right ear was 0.57, which means the higher levels of immunoglobulin M (IgM) specific Cytomegalovirus, the higher dB wave V the ABR results. This pattern can be seen from the scatterplot diagram (Figure 1). The result of the left ear ABR obtained a correlation coefficient of 0.58 which means the higher the level of specific immunoglobulin M (IgM) Cytomegalovirus, the higher dB wave V the ABR results (Figure 2). The above patterns can be explained in the presence of cytomegalovirus infection which occurs during pregnancy, when the virus has begun to infect the fetus, so that when the baby is born the examination will find an increase in IgM levels of Cytomegalovirus. Hearing loss in patients can be caused by the presence of various factors. The first factor is the presence of intracerebral infection which causes brain microcephaly, ventricular calcification, and body weight loss. The second factor involves a disruption in the hair cell which is associated with an infection in the cochlea, while the latter is an immune response to the congenital infection.
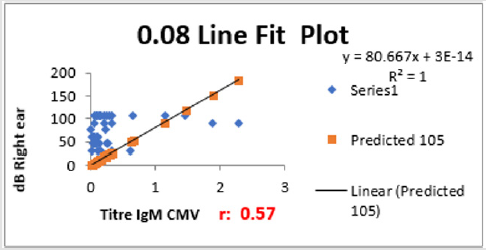
Figure 1: The scatterplot diagram and correlation coefficient (r) between Cytomegalovirus Specific Immunoglobulin M and dB wave V right ear.
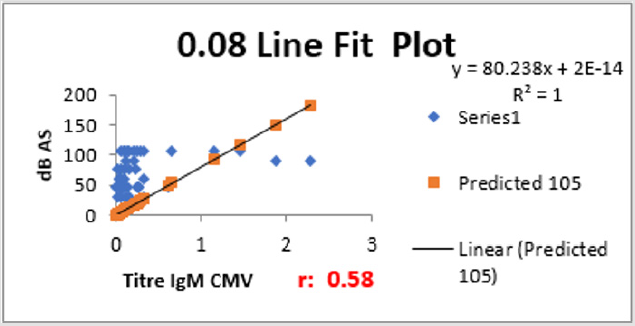
Figure 2: The scatterplot diagram and correlation coefficient (r) between Cytomegalovirus Specific Immunoglobulin M and dB wave V left ear.
In developing nations with highly seropositive populations, prevalence ranges between 1% and 6%. This correlation is explained by the fact that cCMV birth prevalence increases with maternal seroprevalence [17]. Schachtele et al. stated that when there was a viral infection in the intracerebellar, infiltration of the cochlea and surrounding tissue, and immune response can contribute to the onset of hearing loss caused by cCMV infection. Hair cell disorders in patients can also be caused by an inflammatory reaction from the cochlea [10]. Pass et al. mentioned that Cytomegalovirus can infect nerve progenitor cells and disrupt the process of growth and differentiation.
Conclusion
Based on the results of this study, it can be concluded that there is a strong correlation between dB V wave appearance from ABR examination with Cytomegalovirus-specific levels of immunoglobulin M (IgM) in patients with congenital Cytomegalovirus infection.
Acknowledgement
We are gratefully indebted to our study participants in Yogyakarta. We also express our gratitude to the Perinatology Division Staff, Dr. Sardjito General Hospital and all research assistants (ENT Residents and Nurses) who participated in this research, and to the Health Research Ethics Committee Faculty of Medicine Universitas Gadjah Mada that gave permission, license and approved this research.
References
- Long SS, Prober CG (2018) Principles and Practice of Pediatric Infectious Diseases. 5th
- Ross SA, Novak Z, Pati S, Boppana SB (2011) Overview of the diagnosis of cytomegalovirus infection. Infect Disord Drug Targets 11(5): 466-474.
- Yamamoto AY, Mussi-Pinhata MM, De Lima Isaac M, Rezende Amaral F, Carvalheiro CG, et al. (2011) Congenital cytomegalovirus infection as a cause of sensorineural hearing loss in a highly immune population. Pediatr Infect Dis J 30(12): 1043-1046.
- Pass RF (2018) Cytomegalovirus. In L Sarah S C G Prober & F Marc eds Principles and Practice of Pediatric Infectious Diseases. Philadelphia: Else: 5569-5608.
- Wood SA, Sutton GJ, Davis AC (2015) Performance and characteristics of the Newborn Hearing Screening Programme in England: the first seven years. Int J Audiol 54(6): 353-358.
- Pitlick MM, Orr K, Momany AM, McDonald EL, Murray JC, et al. (2015) Determining the prevalence of cytomegalovirus infection in a cohort of preterm infants. J Neonatal Perinatal Med 8(2): 137-141.
- Hanshaw JB (2006) Congenital cytomegalovirus infection: laboratory methods of detection. J Pediatr 75(6): 1179-1185.
- Mizuno T, Sugiura S, Kimura H, Ando Y, Sone M, et al. (2009) Detection of cytomegalovirus DNA in preserved umbilical cords from patients with sensorineural hearing loss. Eur Arch Otorhinolaryngol 266(3): 351-355.
- Shin SH, Suh MW, Chang MY, Choi EH, Kim HS, et al. (2018) Characterization of detailed audiological features of cytomegalovirus infection: a composite cohort study from groups with distinct demographics. Biomed Res Int: 1-8.
- Schachtele SJ, Mutnal MB, Schleiss MR, Lokensgard JR (2011) Cytomegalovirus-induced sensorineural hearing loss with persistent cochlear inflammation in neonatal mice. J Neurovirol 17(3): 201-211.
- Wang Y, Patel R, Ren C, Taggart MG, Firpo MA, et al. (2013) A comparison of different murine models for cytomegalovirus induced sensorineural hearing loss. Laryngoscope 123(11): 2801-2806.
- Fowler KB, McCollister FP, Sabo DL, Shoup AG, Kris E Owen KE, et al. (2017) Targeted approach for congenital cytomegalovirus screening within newborn hearing screening. Pediatrics 139(2): 1-7.
- Teissier NS, Quesnela BS, Van Den Abbeele T (2016) Audiovestibular consequences of congenital cytomegalovirus infection. Eur Ann Otorhinolaryngol Head Neck Dis 133(6): 413-418.
- https://www.ncbi.nlm.nih.gov/pubmed/24257422
- Marsico C, Kimberlin DW (2017) Congenital cytomegalovirus infection: advances and challenges in diagnosis, prevention and treatment. Ital J Pediatr 43:38: 1-8.
- Goderis J, Els De Leenheer, Smets K, Van Hoecke H, Keymeulen A, et al. (2014) Hearing loss and congenital CMV infection: a systematic review. Pediatrics 134 (5): 972-982.
- Lanzieri TM, Dollard SC, Bialek SR, Grosse SD (2014) Systematic review of the birth prevalence of congenital cytomegalovirus infection in developing countries. Int J Infect Dis. 22: 44-48.
