 Case Report
Case ReportAbstract
Infectious mononucleos is an Epstein-Barr virus (EBV)-induced disease prevalent during preadolescence, predominantly has highly elevated lymphocytosis with a more than 10% share of atypical lymphocytes. We presented a case of an adult who developed concurrent Epstein-Barr virus and three atypical pathogens infections. And in this case, eosinophils were increased significantly while lymphocytes were normal and the test of atypical lymphocytes is negative, which are very rare in EBV Infectious mononucleosis.
Keywords: Infectious Mononucleosis; Epstein-Barr Virus; Massive Eosinophils; Co-Infection; Atypical Pneumonia; Mycoplasma Pneumoniae; Chlamydia Pneumoniae; Legionella Pneumophila
Abbreviations: CT: Computed Tomography; EBV; Epstein-Barr virus; LP: legionella Pneumophila; VCA: Viral Capsid Antigen; MP: Mycoplasma Pneumoniae; CP: Chlamydia Pneumoniae
Case Report
A 28-year-old man had a one-month history of fever, mild cough, and abdominal distension. He was started on cephalosporin antibiotic for the suspicion of upper respiratory infections but returned to our hospital one week later with continued fevers. On admission the patient had a high fever of 39.2°C. Physical examination revealed enlarged pharyngeal tonsils, bilateral inguinal lymphadenopathy and slight epigastric tenderness. Cephalosporin and antipyretic were ineffective for improving his clinical symptoms. His body temperature ranged from 38.2℃ to 39.2℃. Laboratory analysis showed high leucocytosis (22.93× 109/L with 73.8% eosinophils and no atypical lymphocytes) (Figure 1), mildly elevated liver enzymes (alanine transaminase, 83 U/l). Laboratory testing was negative for mycobacterium tuberculosis, viral hepatitis A, B, C, D and E, influenza, dengue, leptospira, epidemic hemorrhagic fever, cytomegalovirus, Herpes simplex virus, typhoid fever, Liver fluke, autoimmune antibody, parasites, blood culture and bone marrow. Ultrasound showed left neck, bilateral inguinal, liver and peripancreatic region lymphadenopathy. Chest and abdominal computed tomography (CT) scan revealed left upper-lobe infiltrates, multiple small areas of low density in liver parenchyma (Figures 2 & 3). Liver biopsies identified acute inflammation of huge amounts of eosinophils (Figure 4).
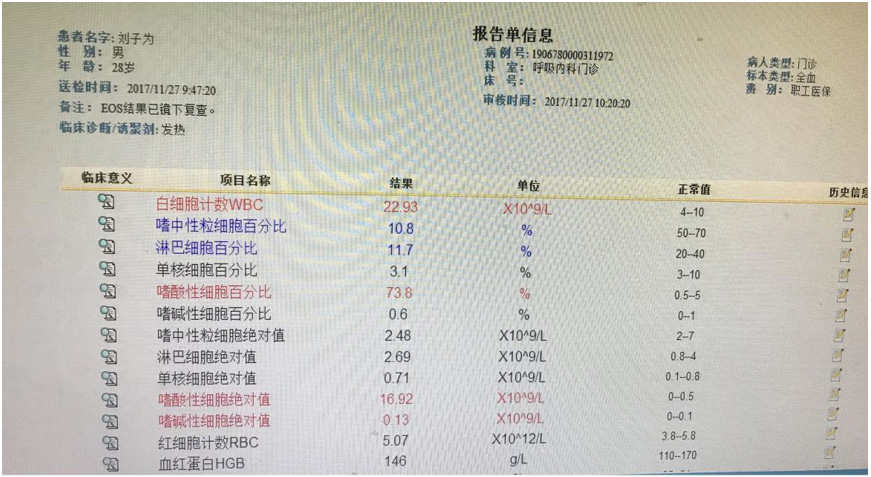
Figure 1: Blood test on November 27, 2017 (high leucocytosis (22.93× 109/L) with 73.8% eosinophils).
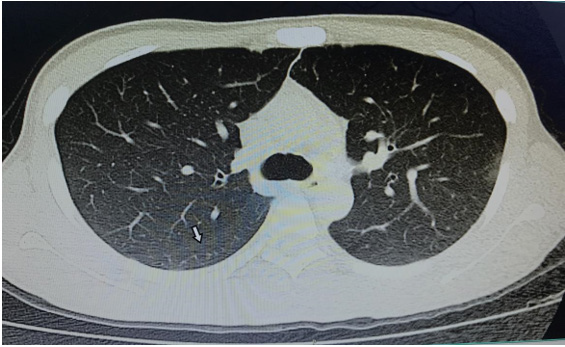
Figure 2: Chest CT enhancement scan (left upper-lobe infiltrates).

Figure 3: Enhanced CT of abdomen (multiple small areas of low density in liver parenchyma).
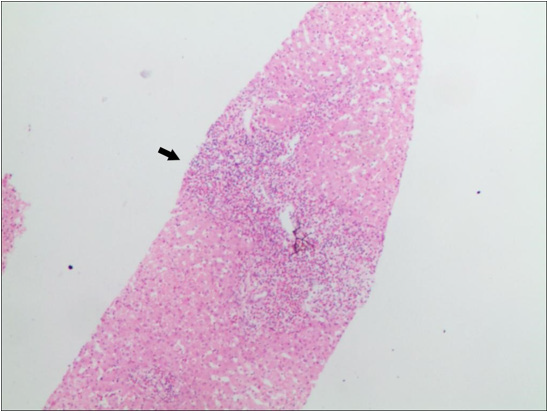
Figure 4: Liver biopsy (acute inflammation of huge amounts of eosinophils).
These findings preliminarily excluded rheumatic diseases, parasitic diseases, the common virus infection, hematologically related diseases and tumors. To determine the cause of fever, interrelated tests of other unusual pathogens were examined further. IgM antibodies to Epstein-Barr virus (EBV) viral capsid antigen (VCA), Mycoplasma pneumoniae (MP), Chlamydia pneumoniae (CP) and legionella pneumophila (LP) were positive, suggesting multiple infection. EBV DNA was positive (5.4×105 copy/ml) while heterophil agglutination test was negative. Based on these clinical features and serological studies, the patient was diagnosed with infectious mononucleosis (IM) and communityacquired pneumonia caused by three atypical pathogens (MP, CP, LP). Therefore, the patient was started on anti-infective therapy with ganciclovir, erythromycin and ciprofloxacin. After four days his temperature dropped to normal and then he was discharged and monitored in the outpatient clinic. At the five-week follow-up, his white blood cells and eosinophil were completely normal.
Discussion
Infection mononucleosis (IM) is an acute infectious disease which is caused by EBV, spreads through droplet and usually occurs during preadolescence. Clinical presentations are composed of nonspecific symptoms, including fever, sore throat, lymphadenopathy, splenomegaly and hepatomegaly [1]. High lymphocytosis with atypical lymphocytes is highly suggestive of EBV IM, and elevated IgM antibodies and EBV DNA is the most accurate method to confirm the diagnosis. Although IM is a self-limiting illness, it can involve many important organs and systems and vary greatly in symptoms, which lead to its high misdiagnosis rate. Antibiotics were ineffective and this was the reason why fever had been continued until an antiviral drug was given. Pneumonia caused by atypical pathogens, including MP, CP and LP can be called Atypical pneumonia [2]. It can be confirmed by symptoms (fever, sore throat, cough, and so on), blood picture (reduced or normal leucocyte), chest radiograph and the detection of atypical pathogens specific antibodies (positive IgM antigens).Here, we presented an exceptional case of IM which has the following characteristics:
a) As a 28-year-old healthy adult, the clinical presentation
and positive EBV, MP, CP and LP IgM test strongly suggested
four pathogens co-infection. No prior case report has described
similar scenarios.
b) Though he had typical clinical findings of EBV IM like
fever, sore throat and lymphadenopathy, his blood test showed
normally lymphocytosis with no atypically lymphocytes and
massive eosinophils. It is really rare in IM, only two analogous
cases have been reported previously by searching related case
reports [3]. Eosinophils in these two cases was only one- eighth
of our case. Based on laboratory analysis and CT findings, the
patient was excluded differential diagnosis which have high
eosinophilia, such as parasitic infection, anaphylaxis, rheumatic
diseases, blood system diseases and tumor, and confirmed that
massive eosinophilia was the response to mixed infections(EBV,
MP, CP and LP) [4]. Failed treatment of common antibiotics and
effectivity of antiviral drug and targeted anti-infection drugs
were consistent with the diagnosis.
c) This patient was simultaneously infected by four
pathogens and diagnosed with four diseases. It is one of its
characteristics. We guessed that the patient was infected by
one or two types of pathogens first, and the initial infection and
decreased immunity and defense function rendered the host
more susceptible to co-infection. Atypical pathogens infections,
such as EBV, mycoplasma, chlamydial, legionella, dengue
and cytomegalovirus usually involve different organs and
systems, and therefore the clinical presentations in patients
infected with multiple pathogens can vary greatly. In order to
avoid misdiagnosis, to obtain early recognition and to give a
timely treatment to facilitate a full recovery, it is essential to
do comprehensive detection of atypical pathogens earlier for
patients presenting with continued fever, atypical symptoms or
blood picture and void routine therapy.
References
- Xie Zhengde (2007) Clinical features and diagnostic criteria of infectious mononucleosis associated with Epstein-Barr virus infection in children. Appl Clin Pediatr 22(22): 1759-1760.
- Tong Chuntang, Chen Hangwei (2014) Research development on the diagnosis of atypical pathogens in community acquired pneumonia. Chin J Lung Dis 7(6): 675-678.
- Wang Tao, Wang Yazhen (1990) Two case reports of Infectious mononucleosis with increasing eosinophils. The Liao Ning Journal of Medicine (3): 149-150.
- Lin Jie, Wu Yongji (2005) A clinical analysis of 53 cases of hypereosinophilia. Chinese Journal of Practical Medicine 25(11): 1017- 1018.
