 Mini Review
Mini ReviewAbstract
The Ashman phenomenon is aberrant ventricular conduction that usually seen in atrial fibrillation. It does not require a specific treatment; it is usually treated according to the underlying cause. Differential diagnosis is important. It should be well distinguished from the other arrhythmias. Because the treatment and prognosis can vary considerably.
Keywords: Ashman Phenomenon; Aberrant Conduction; Electrocardiography
Introduction
Ashman phenomenon is an aberrancy of ventricular conduction as a result of a change in the QRS cycle length. It is typically seen in AF. However, it may also occur in other supraventricular tachyarrhythmias. First reported by Gouaux and Ashman in 1947. In atrial fibrillation, when a long cycle was followed by a relatively short cycle, they showed that a short cycle beat often had a right Bundle Branch Block (RBBB) morphology [1]. Although the Ashman phenomenon is more than sixty years, it is still often not recognized or is misdiagnosed as PVC [2]. Understanding the Ashman phenomenon is useful and necessary in daily clinical practice. because, for example, in the 24-hour Holter ECG records, we can even find thousands of large QRS complexes caused by the Ashman phenomenon.
Pathophysiology
The Ashman phenomenon is an intraventricular conduction disorder. The aberrant conduction depends on the heart rate and the relative refractory period of the conduction tissue components. The refractory period duration of myocytes is directly proportional to the R-R interval of the previous cycle. This means that the shorter action potential time is associated with a shorter R-R interval, and the longer action potential time is associated with a longer R-R interval. If a short R-R interval occurs after a long cycle, the refractory period will also extend, and a supraventricular warning earlier than the previous one will catch one of the rights and left branches during the refractory period, and it is likely to be transmitted by aberration. When an impulse achieves the HisPurkinje fibres, the aberrant conduction occurs when one of its branches is still in the absolute or relative refractory period. In this case, it causes blocked conduction in the branching area and delays the depolarization through the ventricular muscles. Eventually, in the absence of bundle-branch pathology, it causes a bundle-branch block morphology in the surface Electrocardiogram (ECG). The right bundle branch has a longer refractory period. Therefore, the RBBB pattern is more common in the Ashman phenomenon.
The Ashman phenomenon is a common ECG finding in clinical practice and it’s associated with underlying pathology. In clinical trials, the Ashman phenomenon alone is asymptomatic and does not require any specific treatment. Mortality and morbidity depend on the underlying pathology.
Causes
The Ashman phenomenon is seen in cases that cause changes in the duration of the refractory period of ventricular tissue or bundle branch. These cases are usually atrial fibrillation, atrial tachycardia and atrial ectopy. A previous study showed that dofetilide, which can be used to control rhythm in atrial fibrillation, supports the development of the Ashman phenomenon. Dofetilide blocks the repolarization of the cell by blocking the potassium channels in phase 3 of the action potential and prolongs the plateau phase of the action potential. As a result, the Ashman phenomenon emerges with the prolongation of the ventricular refractory period. The study included 10 patients with atrial fibrillation. Patients were given 250-500 micrograms of dofetilide every 12 hours after the loading dose. They found that total Ashman beats increased from 42 ± 24 prior to dofetilide administration, 93 ± 79 after the first dose of the drug, and 133 ± 101 after the second dose [3].
Differential Diagnosis
Understanding the Ashman phenomenon is helpful in distinguishing aberrant supraventricular arrhythmias from wide complex arrhythmias of ventricular origin. Because the prognosis and treatment practices are very different from each other. An aberrant conducting supraventricular impulse may be miscible with a PVC.
Diagnosis
There are no specific physical examination findings. Fisch criteria [4] are used to diagnose the Ashman phenomenon:
a) Relative long cycle instantly antecedent the cycle ended by the aberrant QRS complex: Aberrations can be seen on both RBBB and LBBB patterns. The short-long-short interval is more possible to start aberration.
b) RBBB-shaped aberration with the normal orientation of the first QRS vector:
c) Irregular coupling of aberrant QRS complexes
d) Absence of fully compensatory pause
The morphology of QRS is the most useful clue of distinguishing between a supraventricular and ventricular source of wide QRS complexes. Morphological features supporting the ventricular origin of wide complexes are:
a) Slurred or crenated downstroke with LBBB morphology in leads V1 or V2
b) RBBB morphology with monophasic R, biphasic QRS, or rSR’ pattern in lead V1.
c) QS pattern in lead V6.
d) QRS duration in LBBB morphology is longer than 160 milliseconds and QRS duration in RBBB morphology is longer than 140 milliseconds
e) In a precordial lead, RS interval longer than 100 milliseconds
f) •Evident left axis (between -90° and 180°) (Figure 1).
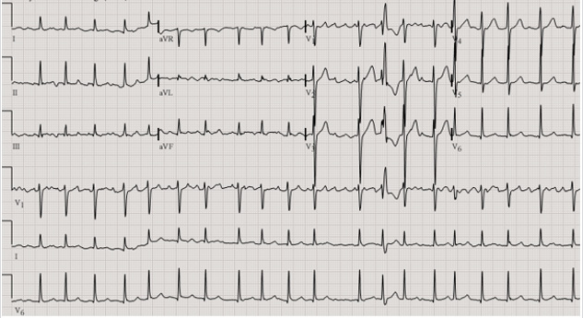
Figure 1: Ashman phenomenon illustrated in atrial fibrillation ECG.
Conclusion
As a result, it is necessary to know the Ashman phenomenon in order to avoid unnecessary diagnosis and more important treatment procedures in a patient with large QRS complexes with atrial fibrillation and RBBB morphology.
References
- Gouaux JL, Ashman R (1947) Auricular fibrillation with aberration stimulating ventricular paroxysmal tachycardia. Am Heart J 34: 366.
- Kennedy LB, Leefe W, Leslie Br (2004) The Ashman phenomenon. J La State Med Soc 156: 159-162.
- Sardar MR, Khaji A, Robert J, Bradley JT, Yan G (2013) Abstract 10380: The Ashman phenomenon in patients with atrial fibrillation treated with an IKr Blocker, Dofetilide. Circulation Vol. 128.
- Fisch C (1983) Electrocardiography of arrhythmias: From deductive analysis to laboratory confirmation--twenty-five years of progress. J Am Coll Cardiol 1(1): 306-316.
