 Mini Review
Mini ReviewAbstract
Clomiphene, one of selective estrogen receptor modulator, indirectly induces ovulation. It stimulates the secretion of pituitary gonadotropins and thus increases circulating testosterone levels. These hormonal effects may be responsible for the patient’s unfavorable psychotic outcomes in concert with clomiphene’s anti-estrogen activity. Infertile women, in particular those with a prior psychiatric episode, taking clomiphene is associated with high frequencies of psychological side effects. Clomiphene induces mood instability in 60-70% of the cases and more serious changes are very rare. The commitment of the attending gynecologists to become familiar with and identify psychological problems may lead to the detection at an early and curative stage and potentially counseling the patients to discontinue taking clomiphene.
Keywords: Clomiphene; Ovulation Induction; Psychiatric Illness, Mood Swings; Androgen.
Introduction
Clomiphene citrate belongs to the selective estrogen receptor modulator (SERM) and has been used as an ovulation inducer for decades [1,2]. It affects the hypothalamus-pituitary-gonadal axis and indirectly stimulates the production of pituitary gonadotropins, follicle-stimulating hormone (FSH) and luteinizing hormone (LH), and subsequently testosterone level. The wide usage of the clomiphene citrate raises a question whether it induces unfavorable psychotic outcomes or not. In normal healthy women, clomiphene induces mood instability in 60-70% of the cases (Table 1). However more serious changes of mood and awareness are very rare. Therefore, this paper aims to highlight some hormonal effects, as it is not yet understood, which may be responsible for the patient’s psychotic state.

Table 1: Clinical studies on clomiphene-induced psychological side effects in female.
Literature review
In a literature review we found 7 single case reports of psychosis secondary to clomiphene therapy in female (Table 2). Many (5 of 7) case repots have a known psychiatric history; but 2 cases do not (Table 2). In these 2 cases, it is likely that a remote preceding episode of subclinical psychiatric issue may have been unreported. For many patients, a former history of mental illness (e.g. bipolar affective disorder and depression) can be subtle if not exhaustively explored, such as the history of transient neurological dysfunction [3] or preceding suicide attempt and lifetime psychotic instability [4]. Grimm and Hubrich [5] describe the case with paranoid delusion even one day after the beginning of clomiphene therapy. In all cases, the temporal association of both the onset and resolution of their symptoms with clomiphene initiation (or during treatment) and discontinuance, respectively, it is plausible to conclude that the development of psychiatric symptoms results from clomiphene treatment.
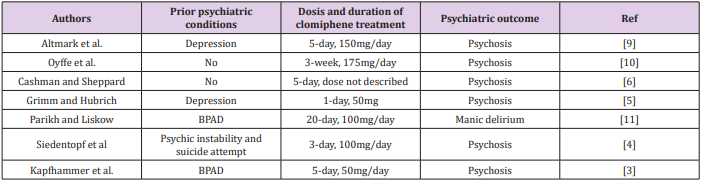
Table 2: Case reports of psychosis with clomiphene therapy in female.
BPAD: bipolar affective disorder.
Comments
Clomiphene citrate-associated psychotic states may be induced in an analogous manner to estrogen-withdrawal psychosis, a condition observed in peri- and post-menopausal women [6]. A rapid decrease in estrogen activity might lead to drastic changes in neurotransmission. As alternative plausible mechanism of clomiphene-induced psychotic symptoms, by causing negative feedback of estrogen receptor, clomiphene indirectly enhances LH and FSH releases, which ultimately results in increased testosterone levels. An enhanced testosterone-androgen receptor interaction in the brain subsequently changes the emotional conditions. Proposed neurobiological targets include catecholaminergic cells in the hypothalamus and other brain limbic regions [7-11]. The complexity and heterogeneity in this mode account for the broad variety of psychiatric symptoms documented in the future aspects. Patients with an underlying psychiatric history may be particularly wounded to the psychological side effects of clomiphene. Further and large-scale studies are waited to accumulate evidence in greater numbers of cases in further evaluating the potential risks of psychiatric complications associated with clomiphene therapy. The commitment of the attending gynecologists to become familiar with and identify psychological problems may lead to the detection at an early and curative stage and potentially counseling the patients to discontinue taking clomiphene.
References
- Yilmaz S, Yolmaz Sezer N, Gönenç IM, Ilhan SE, Yilmaz E (2018) Safety of clomiphene citrate: a literature review. Cytotechnology 70(2): 489-495.
- Davidson R, Motan T, Korownyk C (2016) Clomiphene for anovulatory infertility. Can Fam Physician 62(6): 492.
- Kapfhammer H, Messer T, Hoff P (1990) Psychotic illness during treatment with clomifen. Dtsch Med Wochenschr 115(24): 936-939.
- Siedentopf F, Horstkamp B, Stief G, Kentenich H (1997) Clomiphene citrate as a possible cause of a psychotic reaction during infertility treatment. Hum Reprod 12(4): 706-707.
- Grimm O, Hubrich P (2008) Delusional belief induced by clomiphene treatment. Neuropsychopharmacol Biol Psychiatry 32(5): 1338-1339.
- Cashman F, Sheppard R (1982) Clomiphene citrate as a possible cause of psychosis. Can Med Assoc J 126(2): 118.
- Choi S, Shapiro H, Robinson GE, Irvine J (2005) Psychological sideeffects of clomiphene citrate and human menopausal gonadotrophin. J Psychosom Obstet Gynaecol 26(2): 93-100.
- Blenner J (1991) Clomiphene-induced mood swings. J Obstet Gynecol Neonatal Nurs 20(4): 321-327.
- Altmark D, Tomer R, Sigal M (1987) Psychotic episode induced by ovulation-initiating treatment. Isr J Med Sci 23(11): 1156-1157.
- Oyffe I, Lerner A, Isaacs G, Harei Y, Sigal M (1997) Clomiphene-induced psychosis. Am J Psychiatry 154(8): 1169-1170.
- Parikh A, Liskow B (2007) Manic delirium associated with clomipheneinduced ovulation. Psychosomatics 48(1): 65-66.
