 Research Article
Research ArticleAbstract
Introduction: When an operator performs a study of diaphragmatic function by ultrasonography, it is interesting to record the breathing cycle.
Methods: This work reports the development of a device making it possible to transmit the signal of the beginning of inspiration and expiration to the ultrasound machine via ECG cables.
Results: The monitoring of respiratory function using a turbine spirometer provided the simultaneous measurement of the gas volume and the breathing rate. The device is usable with any commercial ultrasound machine and the cost of manufacture is low (about €70- $82).
Discussion: The device developed by our team will enable further innovative studies. The study of the diaphragmatic deformation using speckle tracking imaging can be triggered by the breathing cycle. The combination of the measurement of the gas volume per cycle with the corresponding diaphragmatic thickening or displacement leads to the possibility of assessing the respiratory work.
Keywords: Chest; Ultrasonography; Diaphragmatic Motion; Diaphragmatic Thickness; Speckle Tracking Imaging
Abbreviations: US: Ultrasonography; 2D: Two-Dimensional; STI: Speckle Tracking Imaging; LCD: Liquid Crystal Display
Introduction
In recent years, several works have supported the significance of ultrasonography in the assessment of diaphragmatic function [1,2]. The excursions of both hemidiaphragms can be measured by M-mode ultrasonography (US). Normal values of diaphragmatic motion have been reported [3] and M-mode US is able to detect hemi diaphragmatic paralysis or hypokinesis [4-6]. In patients suffering from neuromuscular disease, the measurement of diaphragmatic excursion during forced breathing can predict an impairment in vital capacity [7]. Two-dimensional ultrasonography (B-mode US) makes it possible to measure diaphragmatic thickness at various breathing time such as the end of normal expiration (functional residual capacity), at the end of normal inspiration and at total pulmonary capacity [1]. B-mode US has demonstrated its importance in the diagnosis of diaphragm paralysis [8] and of diaphragm dysfunction in patients suffering from myopathy [9]. Some studies have suggested that speckle tracking ultrasound (STI) was superior to conventional ultrasound techniques [10].
It has been reported that the diaphragmatic parameters measured by STI were related to the measurements performed by M-mode US and B-mode US [11,12]. STI might provide more clarification via the analysis of the longitudinal muscle deformation [13]. Unfortunately, no ultrasound machine has been developed to study diaphragmatic strain. The software used in these circumstances is the software designed to track 2D speckle motion in echocardiograms. Consequently, during the STI analysis of the diaphragm, the tracking time is related to a cardiac cycle time period and not to the breathing cycle. To study the maximum deformation of the diaphragm it would be important to analyses the diaphragm during the entire inspiratory phase. The aim of this work was to develop a system enabling the recording of the respiratory signals on the ultrasound machine.
Methods
The specifications of the device were initially determined: To improve the quality of the analysis of the diaphragmatic function by ultrasonography, it would be useful to record the beginning of inspiration and expiration on the screen of the ultrasound machine and to measure simultaneously the gas volume and the ultrasonographic parameters (hemi diaphragmatic excursion or muscle thickness). Lastly, the device should be usable with any commercial ultrasound machine.
Results
Figure 1 reports the principle of the device developed to record breathing signals on ultrasound machines. Monitoring of the breathing rate and gas volume was performed using a commercially available turbine spirometer (price about €1.6 - $1.9, Flow Mir, Medical International Research, Rome, Italy). The turbine support was built using a three-dimensional printer. This support incorporated 3 sensors (1 infrared led and 2 infrared phototransistors, price: €10 - $11.6) to detect breathing time and assess gas volume. The number of turbine rotations was counted by the sensors to assess the gas volume. The direction of the rotation made it possible to distinguish inspiration and expiration. A microcontroller (Nano, Arduino, price: €25 - $29) was used to acquire and interpret the sensor signals.
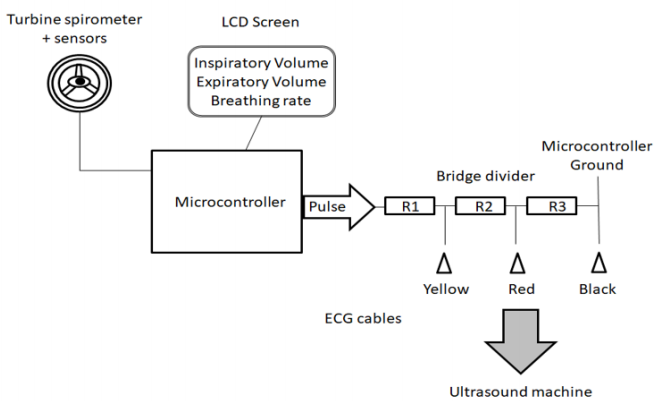
Figure 1: Principle of the device developed to record breathing signals on the ultrasound machines.
The breathing parameters (inspiratory and expiratory volumes, breathing rate) were displayed on an LCD screen (price: €33 - $38). Furthermore, electronic signals were sent to the ultrasound machine via ECG cables. To record the beginning of inspiration and expiration, a voltage pulse was sent now of the reversion in the rotational direction of the turbine. The duration of the voltage pulse was adjustable (from 500 to 1200 microseconds) and transmitted by the microcontroller to a bridge voltage divider. This bridge divider made it possible to decrease the voltage to 50mV to the first electrode and to 25mV to the second electrode. Consequently, the signal amplitude recorded on the screen of the ultrasound machine differed according to the breathing time i.e. inspiration and expiration (Figure 2). The system was powered via the USB connection of the ultrasound machine.
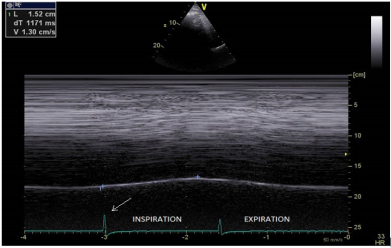
Figure 2: Measurement of the diaphragmatic excursion (1.52cm) during quiet breathing, by M mode ultrasonography: the voltage pulse reports the beginning of both inspiration (arrow: larger voltage) and expiration (image produced using a Vivid E90 and a M5S transducer, GE Healthcare, Little Chalfont, United Kingdom).
Abbreviations: L: diaphragmatic excursion in cm, dT: duration of the diaphragmatic contraction in ms, V: velocity of contraction in cm/s.
Discussion
The advantage of the device was to record simultaneously the breathing cycle via the ECG cables and the diaphragmatic images by ultrasonography. The device developed by our team is of interest for several supplementary reasons. The cost of manufacture is low, in total about €70 - $82, including the turbine spirometer, the sensors, the microcontroller and a screen. No change to the ultrasound machine is needed since the transfer of the signals is transmitted via ECG cables. Consequently, the device is suitable for application with any commercially available ultrasound machines. M-mode ultrasonography enables the diaphragmatic motion to be measured whereas the two dimensional mode can measure the diaphragmatic thickness in the area of apposition of the diaphragm to the rib cage. The breathing signals on the screen of the ultrasound machine is a guarantee that the measurement is performed at the right breathing time (Figure 3).
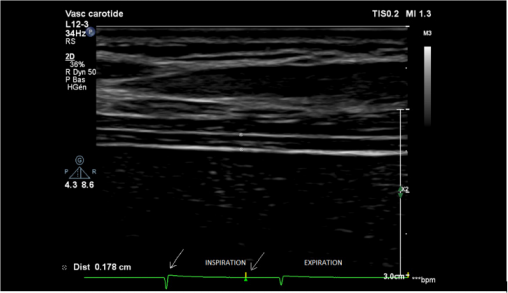
Figure 3: Measurement of diaphragm thickness (d= 0.178cm) in the area of apposition during inspiration (first arrow= beginning of inspiration, second arrow= time of measurement) image produced using a Phillips Affinity 70 Ultrasound system - vascular transducer (L12-3), Koninklijke Philips N.V, Amsterdam, The Netherlands).
In patients suffering from hemidiaphragm paralysis, the signal of the beginning of inspiration can be useful to demonstrate the paradoxical displacement of the paralyzed diaphragm during quiet breathing or deep breathing [6]. The simultaneous measurement of the diaphragmatic motion and the gas volume of the corresponding breathing cycle is also interesting. Indeed, it has been reported on one hand, that the relation between inspired volume and hemi diaphragmatic movement was linear [14] and on the other hand, that diaphragmatic excursions of both sides were quite similar in healthy subjects [3,15]. In patients suffering from hemidiaphragm dysfunction, the right-to-left ratio of maximal excursion on deep breathing can be outside the range of 0.5 to 1.6. In such circumstances, it would be useful to control that the inspired gas volumes corresponding to the diaphragmatic excursions are similar. Furthermore, the work of breathing is the energy expended to inhale and exhale a breathing gas. It can be calculated by the product of the change in thoracic pressure and the change in pulmonary volume.
It has been reported that the measurement of the thickening fraction [the ratio (thickness at inspiration-thickness at expiration)/ thickness at expiration] was related to the transdiaphragmatic pressure–time product per breath [16]. Consequently, the simultaneous recording of the gas volume and the thickening fraction should be useful in assessing the work of breathing. The significance of the study of diaphragmatic function by STI has been recently underlined [13]. The device developed by our team can detect the beginning of inspiration and expiration. Since the information is transmitted to the ultrasound machine via ECG cables, the deformation study by the software can be triggered by the breathing cycle and not by the cardiac cycle. Using this procedure it is possible to perform the analysis of the diaphragm during the entire inspiratory phase (Figure 4).
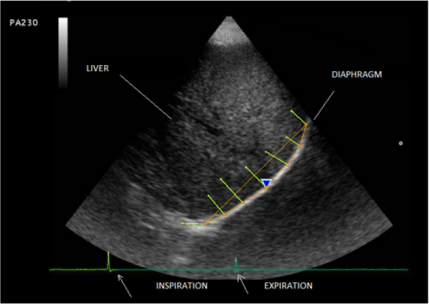
Figure 4: Study of the diaphragmatic deformation triggered by the breathing cycle (first arrow = beginning of inspirationlarger voltage, second arrow= beginning of expiration) - image produced using a Mylab 25 Esaote, Genoa, Italy.
Conclusion
The combination of the recording of the breathing signals and gas volume with the corresponding diaphragmatic thickening or excursion should be useful for a better analysis of the diaphragmatic function.
References
- Costamagna A, Pasero D (2016) Diaphragmatic evaluation in: Emerging Trends in Ultrasound Imaging. SM Group, Dover USA, p. 1-25.
- Cardenas LZ, Santana PV, Caruso P, Ribeiro de Carvalho CR, Pereira de Albuquerque AL (2018) Diaphragmatic ultrasound correlates with inspiratory muscle strength and pulmonary function in healthy subjects. Ultrasound Med Biol 44(4): 786-793.
- Boussuges A, Gole Y, Blanc P (2009) Diaphragmatic motion studied by M-mode ultrasonography: methods, reproducibility, and normal values. Chest 135(2): 391-400.
- Epelman M, Navarro OM, Daneman A, Miller SF (2005) M-mode sonography of diaphragmatic motion: description of technique and experience in 278 pediatric patients. Pediatr Radiol 35(7): 661-667.
- Lloyd T, Tang YM, Benson MD, King S (2006) Diaphragmatic paralysis: the use of M mode ultrasound for diagnosis in adults. Spinal Cord 44(8): 505-508.
- Boussuges A, Brégeon F, Blanc P, Gil JM, Poirette L (2019) Characteristics of the paralyzed diaphragm studied by M-Mode Ultrasonography. Clin Physiol Funct Imaging 39(2): 143-149.
- Carrié C, Bonnardel E, Vally R, Revel P, Marthan R, et al. (2016) Vital capacity impairment due to neuromuscular disease and its correlation with diaphragmatic ultrasound: A preliminary study. Ultrasound Med Biol 42(1): 143-149.
- Gottesman E, McCool FD (1997) Ultrasound evaluation of the paralyzed diaphragm. Am J Respir Crit Care Med 155(5): 1570-1574.
- O Gorman CM, O Brien TG, Boon AJ (2017) Utility of diaphragm ultrasound in myopathy. Muscle Nerve 55(3): 427-429.
- Goutman SA, Hamilton JD, Swihart B, Feldman EL, Rubin JM (2017) Speckle Tracking as a method to measure hemidiaphragm excursion. Muscle Nerve 55(1): 125-127.
- Hatam N, Goetzenich A, Rossaint R, Karfis I, Bickenbach J, et al. (2014) A novel application for assessing diaphragmatic function by ultrasonic deformation analysis in noninvasively ventilated healthy young adults. Ultraschall Med 35(6): 540-546.
- Orde SR, Boon AJ, Firth DG, Villarraga HR, Sekiguchi H (2016) Diaphragm assessment by two dimensional speckle tracking imaging in normal subjects. BMC Anesthesiol 16: 43.
- Oppersma E, Hatam N, Doorduin J, van der Hoeven JG, Marx G, et al. (2017) Functional assessment of the diaphragm by speckle tracking ultrasound during inspiratory loading. J Appl Physiol 123(5): 1063- 1070.
- Houston JG, Angus RM, Cowan MD, McMillan NC, Thomson NC (1994) Ultrasound assessment of normal hemidiaphragmatic movement: relation to inspiratory volume. Thorax 49(5): 500-503.
- Houston JG, Morris AD, Howie CA, Reid JL, McMillan N (1992) Technical report: quantitative assessment of diaphragmatic movement: a reproducible method using ultrasound. Clin Radiol 46(6): 405-407.
- Vivier E, Mekontso Dessap A, Dimassi S, Vargas F, Lyazidi A, et al. (2012) Diaphragm ultrasonography to estimate the work of breathing during non-invasive ventilation. Intensive Care Med 38(5): 796-803.
