 Research Article
Research ArticleABSTRACT
Brief Summary
A low-cost vaginal hysterectomy model is easy to build and would provide an excellent way of reviewing the major landmarks of vaginal hysterectomy.
Abstract
Objectives: To investigate the effectiveness of an educational intervention to teach the basic steps of Vaginal Hysterectomy (VH) to the Obstetrics & Gynecology (OBGYN) residents, using a low-cost model.
Methods: Residents constructed a low-cost VH model, guided by 1 urogynecologist, with step-by-step instructions. Demographics were obtained, followed by assessment on confidence level and knowledge pretest/posttest, and satisfaction survey. Demographics and survey questions were expressed using a descriptive analysis. The test scores were compared within groups using Wilcoxon signed-rank test.
Results: 10 residents participated. The median score from the 10 multiple-choice knowledge questions on the pre-test was 70% [IQR 62.50, 70], while that of post-test was 90% [IQR 80, 90], (p=.013). The range of test score improvement was 0~30% (2 residents improved 0%, 1 resident 10%, 4 residents 20% and 3 residents 30%). Overall, 80% of residents improved their knowledge scores up to 30% after the simulation session. Self-assessed confidence level scores improved from 3 to 4 (1-lowest, 5-highest) in all questions asked. 100% of residents responded with 5 (1-lowest, 5-highest) to the satisfaction statements.
Conclusions: A low-cost VH model increased residents’ confidence and knowledge scores in performing VH. This low-cost VH model can serve as an alternative method to teach the basic steps of VH to the OBGYN residents.
Introduction
Vaginal hysterectomy (VH) is the preferred route of surgery for benign indications per American College of Obstetricians and Gynecologists (ACOG) [1]. There have been numerous reported benefits to VH when compared to other routes of surgery to include decreased length of hospital stay, decreased operative time, less postoperative pain and quicker recovery [2]. VH also has lower rates of intraoperative and postoperative complications when compared to robotic, laparoscopic and hysterectomies [3]. In addition, VH has the lowest overall cost and is the only minimally invasive route that generates net income [4]. Despite these benefits, there has been a decreasing trend in VH performed although the rate of minimally invasive hysterectomy rates has significantly increased [5]. The overall number of hysterectomies performed/ participated by OBGYN residents has been decreasing with a higher rate of decline for abdominal and vaginal routes [6]. The decline in VH case log numbers translates to less experience for OBGYN residents. According to an online survey, only 38.1% of program directors and 27.8% of residents reported graduating residents as being “completely prepared“ to perform a VH [7].
Simulations certainly have a role in training residents, providing a safe environment for learning and practice, in addition to increasing confidence. Currently, there are VH simulators, but they can be cost prohibitive. For instance, the Miya Model costs $6,700 and its disposable and non-reusable structures cost $440 [8]. There are studies to suggest that low-cost models can also offer improved resident confidence. In a pilot study, 14 residents were able to successfully perform the steps of a VH and confidence was increased using a low-cost model. However, the construction and reloading were time consuming [9]. The objective of this study was to assess efficacy and perceptions of VH simulation using a previously published low-cost model, by Anand (2016) to teach the basic steps of VH to our OBGYN residents. The “no-excuses” VH model was designed to be assembled by the residents under attending’s supervision during an educational session [10,11]. Constructing a low-cost VH model with step-by-step directions, using readily available materials from clinics would allow the OBGYN residents to learn the basic steps of performing VH.
Materials and Methods
The research was conducted during resident teaching sessions at Inspira Medical Center in Vineland, NJ. Inspira Health Institutional Review Board approval (IRB0000285) was obtained. This study with a matched pairs utilized pre/posttest methodology to assess the efficacy and perceptions of VH simulation using a low-cost model, developed by Anand as “the no-excuses“ vaginal hysterectomy model: consisting of structures representing the vagina, uterus, vesicocervical septum, vesicouterine space, peritoneal folds, uterosacral and cardinal ligaments, corneal attachments, bladder, ureters, and rectum using easily accessible supplies from any clinic office, and costing less than US $5 per model.” [10,11]. The required materials to build a low-cost VH model are shown in (Figure 1). In addition to elucidating the relationships of the uterus to its surrounding ligaments and organs, this model emphasizes the anatomic structures critical to achieving safe and effective anterior and posterior colpotomies. To summarize the creation of the model, a uterus was created, to which the uterosacral and cardinal ligaments were attached. The 3 cornual attachments (round ligament, fallopian tube, and uterovaginal ligament) were then applied. The vesicouterine septum was attached, as was the areolar tissue contained in the vesicouterine space. The cervix was threaded into the vagina.
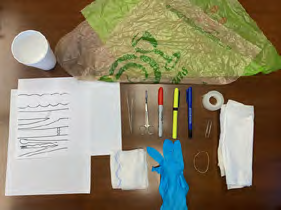
Figure 1: The required materials to build a low-cost VH model.
Note: 2 sheets of A4 plain paper; 2 sheets of plastic bag; 1 yellow highlighter; 1 red pen; 1 foam cup (16 oz); 1 small latex-free glove; 1 square gauze; 2 Kleenex tissues; 1 rubber band; 1 pen; 1 large paper clip; 1 roll scotch tape; 1 pair of scissors and pick up; VH: Vaginal Hysterectomy.
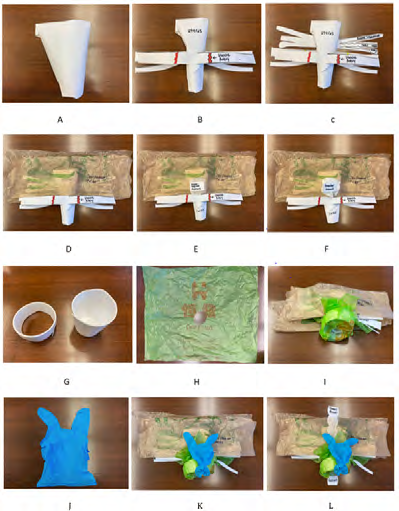
Figure 2: Step-by-step instruction of constructing VH model.
A. Building a paper Uterus.
B. Attaching the uterosacral and cardinal ligaments.
C. Attaching the adnexa and round ligaments.
D. Attaching the peritoneal folds.
E. Attaching the supra vaginal septum.
F. Attaching the areolar tissue.
G. Making the vaginal introitus using a Styrofoam cup rim.
H. Cutting out the plastic bag to make the sheet then cutting out a quarter size circle in the middle to allow the cervix to fit into.
I. Wrapping the plastic sheet around the Styrofoam cup rim to make the vaginal canal then inserting the previously made GYN structure into the cup rim.
J. Making the bladder and ureters by cutting out 1st, 3rd and 5th fingers in the disposable glove.
K. Making the urethra by knotting the glove at the bottom, then attaching it to the anterior portion of the vagina.
L. Attaching small bowel and rectum.
Note: VH: Vaginal Hysterectomy
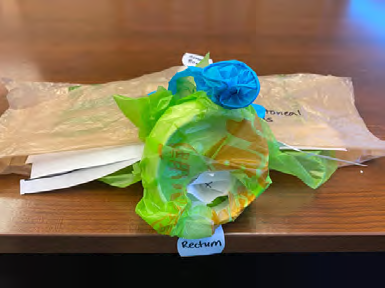
Figure 3: The final presentation of the low-cost VH model.
Note: VH: Vaginal Hysterectomy
The urethra, bladder, and ureters were applied, and the ureters were threaded into the cardinal ligament posterolateral to the representation of the uterine arteries drawn within the cardinal ligament. The rectum was created. The peritoneal folds, including the vesicouterine pouch, the broad ligament, and the rectouterine pouch, were applied. The small intestine was placed intraperitoneally [10,11]. The step-by-step construction directions are shown in (Figure 2). The final presentation of the low-cost VH model is displayed in (Figure 3). A total of 10 OBGYN residents participated in a single 3-hour simulation session with the following sequences:
1. 30 minutes: demographics (Appendix 1), pre-confidence self-test (Appendix 2) and pre-knowledge test (10 multiple choice questions, (Appendix 3).
2. 2 hours: didactics on basic pelvic anatomy building the paper VH model; and reviewing the surgical steps of VH on the model. Each resident built a model in the classroom under direct guidance; and
3. 30 minutes: post-confidence self-test (Appendix 2), postknowledge test (Appendix 3), and satisfaction survey, including a question: how realistic the paper VH model was (Appendix 4). The questionnaires were collected without personal identifiers. Outcomes were measured with the written knowledge test before and after the paper model VH simulation and a selfgraded survey for confidence. The pre-post knowledge tests are validated questions from the ACOG simulation website at https://www.acog.org/education-and-events/simulations/ scog008/quiz.

Appendix 1: Demographics (circle one).
Note: PGY: Post-Graduate Year, VH: Vaginal Hysterectomy, GYN: Gynecology

Appendix 2: Confidence Level Self-Assessment before/after training (1-lowest, 5- highest).
Note: VH: Vaginal Hysterectomy
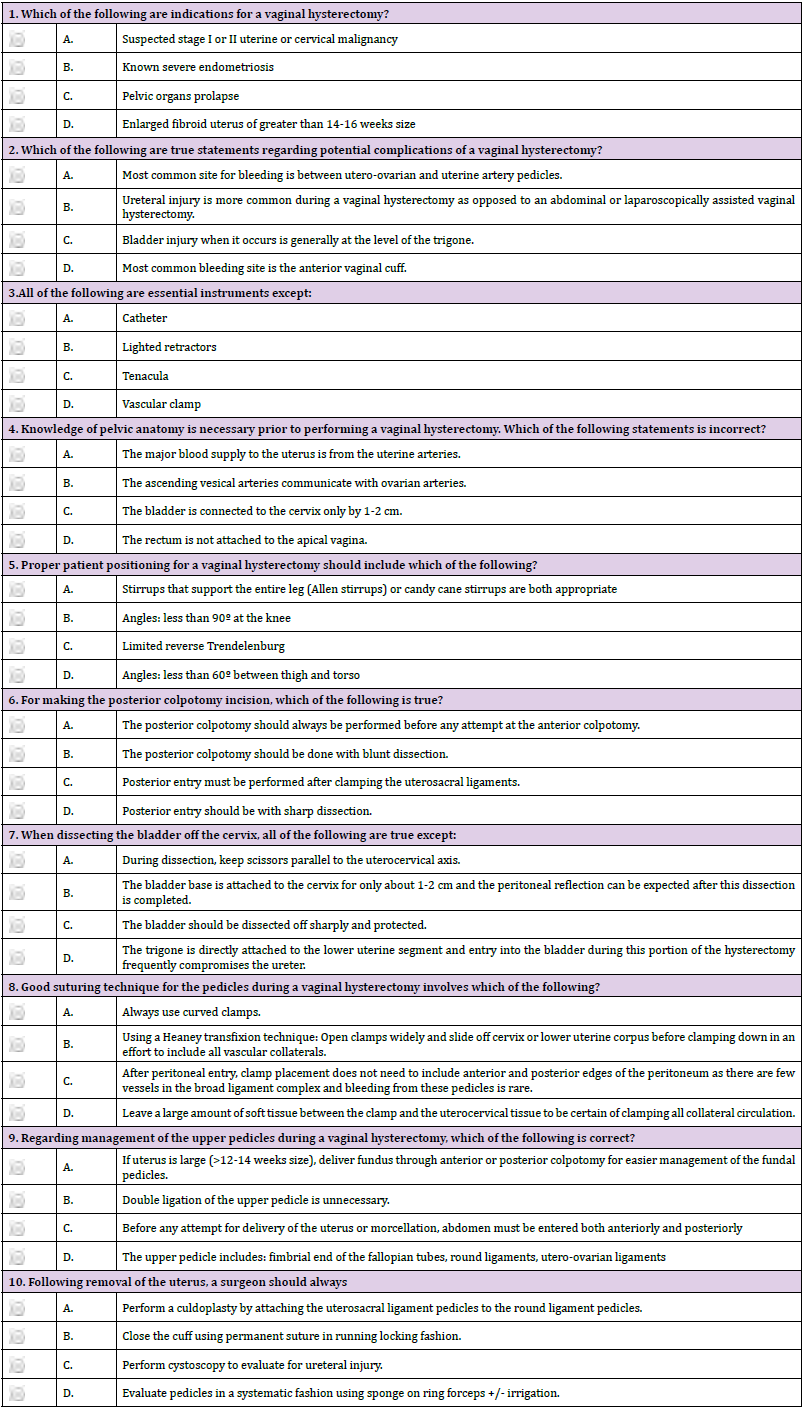
Appendix 3: Pre-Test/Post-Test.

Appendix 4: Satisfaction Survey (1-lowest, 5- highest).
Note: VH: Vaginal Hysterectomy
Statistical Analysis
All analyses were performed using commercially available software: R v.4.0.3 (Vienna, Austria. ISBN 3-900051-07-0, URL: http://www.R-project.org/). The demographic variables and subjectively reported satisfaction survey on the paper VH model were described using descriptive analysis, since there was no control group to compare. The primary outcome was calculated using a bivariate analysis evaluating the written test scores before and after the paper VH simulation. The confidence score in performing VH after the intervention was also compared within the groups as the secondary outcome. Pre- and post-test scores on the written test were compared within groups using the Wilcoxon signed-rank test. All reported p values were 2-sided, and p <0.05 was considered statistically significant.
Results
Of 16 total residents (4 for each PGY level) in our OBGYN residency program, 10 participated the simulation (PGY-1, n=3; PGY-2, n=2; PGY-3, n=3; PGY-4 n=2). 50% of participants were 31- 35 years old, 40% were 26-30 years old, and 10% was more than 36 years old. 60% of residents reported that they had never performed VH, while 40% reported they had performed 1~5 VHs (30%) and 6~10 VHs (10%). (Figure 4) depicts the number of VH performed/participated by the residents. 20% of residents reported they had never observed or participated in VH. 40% of residents had completed more than 10 GYN rotations, 30% completed 6~10 rotations, and 30% completed 1~5 rotations. (Table 1) describes the demographic details.
The median score from the pre-knowledge test was 70% [IQR 62.50, 70], while that of post-knowledge test was 90% ([IQR 80, 90] (p=.013). The range of test score improvement was 0~30% (2 residents improved 0%, 1 resident 10%, 4 residents 20% and 3 residents 30%). Overall, 80% of residents improved the knowledge scores 10-30% after the simulation session. See details in (Table 2). Compared to the residents in PGY 3&4, the residents in PGY 1&2 scored higher in both pre and posttest. (Figure 5) shows the knowledge test score improvement after the simulation in different PGY levels.
Self-assessed confidence level improved from 3 to 4 (1-lowest, 5-highest) in all 3 questions asked: “How well do you feel you know vaginal pelvic anatomy? (p=.010)”, “How well do you feel that you correctly can identify the pelvic landmarks during VH (p=.011)?”, “How confidently do you feel that you understand the basic steps of how to perform a VH? (p=.012)”. (Table 3 & Figure 6) illustrate improvement in self-assessed confidence level after the simulation. On satisfaction survey at the end of the simulation, 100% of residents responded with 5 (1-lowest, 5-highest) to the statements for “the lecture was useful”, “the TVH model was realistic for simulating TVH”, and “The simulation was useful”. See (Table 4).
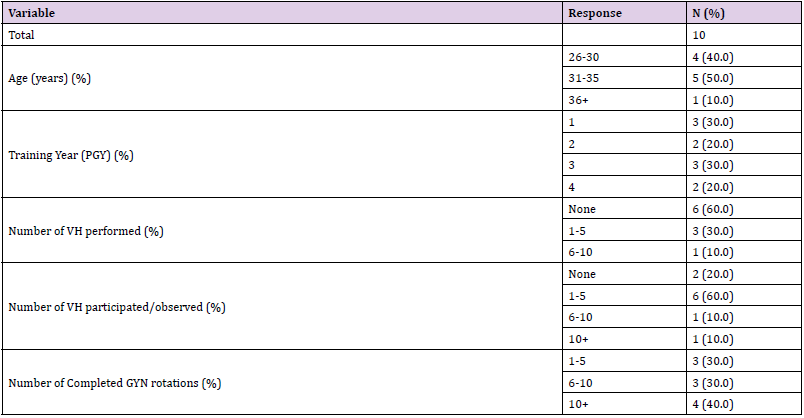
Table 1: Demographics.
Note: PGY: Post-Graduate Year, VH: Vaginal Hysterectomy, GYN: Gynecology

Table 2: Knowledge test scores before and after simulation.
Note: *range in test score improvement is 0 to 30.
IQR: Interquartile range
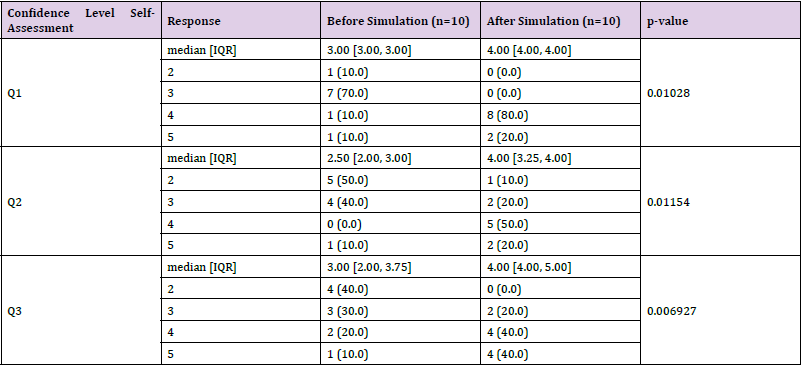
Table 3: Self-assessment of confidence level before and after simulation.
Note: Q1: How well do you feel you know vaginal pelvic anatomy? .
Q2: How well do you feel that you correctly can identify the pelvic landmarks during VH?
Q3: How confidently do you feel that you understand the basic steps of how to perform a VH?
VH: vaginal hysterectomy, IQR: Interquartile range.

Table 4: Satisfaction scores after simulation.
Note: VH: vaginal hysterectomy.
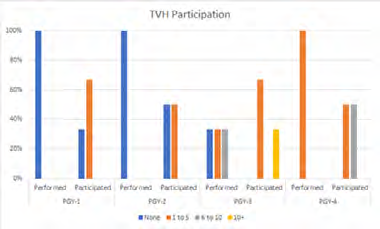
Figure 4: Numbers of Vaginal Hysterectomy Performed/Participated by different PGY levels.
PGY: Post-Graduate Year.
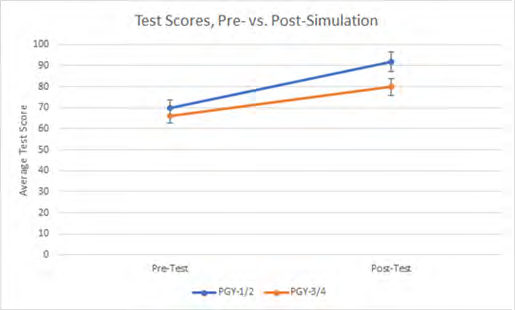
Figure 5: Knowledge Test Score Improvement after the simulation in different PGY levels.
Note: PGY: Post-Graduate Year
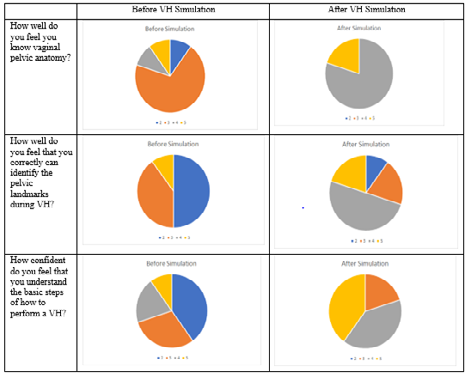
Figure 6: Comparison of self-assessment of confidence level before and after simulation.
Note: VH: vaginal hysterectomy
Discussion
In this study, we described the detailed steps of making the low budget VH model, and how the model increased residents’ confidence and knowledge scores in performing VH. It is wellknown that simulation training enhances the learner’s knowledge on anatomy and basic steps of complex procedures without compromising patient safety. VH is one of the complex procedures that requires knowledge on complex anatomic relationships of vital structures within the relatively restricted space of the bony pelvis: this may limit the ability of teaching VH to the learners [12]. There are several VH simulation models available including Low Fidelity Trainer [9], Miya Model [12], Reusable Pelvic Simulator [13,14]. Almost all the currently available simulators require construction and reloading the parts on the bony pelvis. In addition, they are costly. Unlike them, the low budget paper VH model does not require complex construction or reloading the parts. Furthermore, it costs less than US $5 or even less since all the materials utilized are easy to obtain from the clinic or one’s household. Constructing a low-cost VH model with step-by-step instructions improved OBGYN residents’ knowledge scores and self-assessed confidence level on pelvic anatomy and basic steps of performing VH. In addition, all participants were satisfied with the educational activity.
Limitations of this study include the small number of participants and lack of validation of the low-cost VH model for assessing the residents’ VH skill improvement in the real operative room setting. Although having a valid and reliable simulation model for assessing VH skills is important, it is equally important to have a simulation model for learning VH skills and anatomy relationships in the pelvis. The low budget paper VH model satisfies the latter.
Conclusion
A low-cost VH model increased residents’ confidence and knowledge scores in performing VH. This low-cost VH model can serve as an alternative method to teach the basic steps of VH to the OBGYN residents.
Acknowledgment
The authors acknowledge the low-cost vaginal hysterectomy model was originated from Anand (2016): Anand M. The noexcuses vaginal hysterectomy model. Poster presentation at the American Urogynecologic Society Annual Scientific Meeting; September 27-October 1, 2016; Denver, CO. ePoster 100. Female Pelvic Medicine & Reconstructive Surgery 2016;22(5): S71–S151.
Disclosure
All authors have nothing to disclose.
References
- (2017) Choosing the route of hysterectomy for benign disease. Committee Opinion 701. American College of Obstetricians and Gynecologists. Obstet Gynecol 129: 155-159.
- Aarts J, Nieboer T, Johnson N, Tavender E, Garry R, et al. (2015) Surgical approach to hysterectomy for benign gynaecological disease. The Cochrane Database of Systematic Reviews 8: CD 003677.
- Rahimi S, Jeppson PC, Gattoc L, Westermann L, Cichowski S, et al. (2016) Comparison of perioperative complications by route of hysterectomy performed for benign conditions. Female Pelvic Med Reconstr Surg 22: 364-368.
- Abdelmonem Allam (2006) Observational Comparison of Abdominal, Vaginal and Laparoscopic Hysterectomy as Performed at a University Teaching Hospital. J Reprod Med 51(12): 945-954.
- Kandahari Nazineen , Tucker Lue-Yen , Ojo Anthonia, Zaritsky Eve (2020) Factors Associated With Variation in Vaginal Hysterectomy Rates in an Integrated Health Care System [18B]. Obstetrics & Gynecology 135(23S).
- Gressel Gregory M, Potts John R, Cha Sandolsam, Valea Fidel A, Banks, Erika (2020) Hysterectomy Route and Numbers Reported by Graduating Residents in Obstetrics and Gynecology Training Programs, Obstetrics & Gynecology 135(2): 268-273.
- Burkett D, Horwitz J, Kennedy V, Murphy D, Graziano S, et al. (2011) Assessing current trends in resident hysterectomy training. Female Pelvic Med Reconstr Surg 17: 210-214.
- Guntupalli SR, Doo DW, Guy M, Sheeder J, Omurtag K, et al. (2015) Preparedness of obstetrics and gynecology residents for fellowship training. Obstet Gynecol 126: 559-568.
- Braun Kelli, Henley Barbara, Ray Chadburn, Stager Robert, Rungruang Bunja (2017) Teaching Vaginal Hysterectomy: Low Fidelity Trainer Provides Effective Simulation at Low Cost. Obstetrics & Gynecology 130(44S).
- Anand M (2016) The no-excuses vaginal hysterectomy model. Poster presentation at the American Urogynecologic Society Annual Scientific Meeting; September 27-October 1, 2016; Denver, CO. ePoster 100. Female Pelvic Medicine & Reconstructive Surgery 22(5): S71-S151.
- Anand M, Duffy CP, Vragovic O, Abbasi W, Bell SL (2018) Surgical Anatomy of Vaginal Hysterectomy-Impact of a Resident-Constructed Simulation Model. Female Pelvic Med Reconstr Surg 24(2): 176-182.
- Miyazaki D, Matthews CA, Kia MV, El Haraki AS, Miyazaki N, et al. (2019) Validation of an educational simulation model for vaginal hysterectomy training: A pilot study. Int Urogynecol J 30(8): 1329-1336.
- Barrier BF, Thompson AB, McCullough MW, Occhino JA (2012) A novel and inexpensive vaginal hysterectomy simulator. Simul Healthc 7(6): 374-379.
- Malacarne DR, Escobar EM, Lam CJ, Ferrante KL, Szyld D, et al. (2019) Teaching Vaginal Hysterectomy via Simulation: Creation and Validation of the Objective Skills Assessment Tool for Simulated Vaginal Hysterectomy on a Task Trainer and Performance Among Different Levels of Trainees, Female Pelvic Medicine & Reconstructive Surgery 25(4): 298-304.
