 Research Article
Research ArticleSUMMARY
Purpose of the Study: explore biochemical characteristics of patients with severe complications of diabetic foot syndrome (ulcer, gangrene, amputation) associated with chronic kidney disease.
Research Material: We examined 91 patients (prospectively) with type 2 diabetes with severe complications in the period 2021-2024 at the RSSPMC of Endocrinology, in the department of diabetic foot. All observed patients were divided into 4 groups:
a) 1 gr. – 25 patients with DFS complicated by ulcer, gangrene and amputation and in combination with CKD 4-5 stages on hemodialysis
b) 2 gr. – 25 patients with DFS complicated by ulcer, gangrene and amputation in combination with CKD stages 4-5 without hemodialysis
c) 3 gr - 20 patients with DFS complicated by gangrene and amputation without CKD.
d) 4 gr - 21 patients with DFS, without severe complications, with the initial stage of CKD.
The control group consisted of 20 healthy individuals.
Research Methods: Biochemical (bilirubin, direct, indirect, lipid spectrum, ALT, AST, PTI, coagulogram, blood sugar, glycated hemoglobin, urea, creatinine, GFR, wound pathogens, procalcitonin, interleukin-6, vascular endothelial growth factorVEGF-A and instrumental: ECG, MRI of the feet, Diplography of the main vessels of the legs, ultrasound of the internal organs, the fundus.
Research Results: The highest rates of fasting glycemia were observed in patients of group 2, that is, with DFS and CKD 4-5 stages without hemodialysis. Significantly lower hemoglobin values were also observed in this group of patients (p<0.001), glycated hemoglobin significantly higher values of urea, creatinine and GFR (p<0.001). All patients had significantly reduced values of HDL (p<0.001) and total cholesterol (p<0.05).
Conclusion: Biochemical parameters were significantly impaired in patients of group 1, that is, with DFS and CKD 4-5 stages on hemodialysis, which indicates the need for further research in this group of patients.
Keywords: Type 2 Diabetes Mellitus; Diabetic Foot Syndrome; Chronic Renal Failure; Hemodialysis
Abbreviations: HbA1C: Glycated Hemoglobin; GFR: Glomerular Filtration Rate; P: Significance of Differences Between Groups in Comparison with Control; While P1: Significance of Differences Between Group 1 And Control; P2: Group 2 With Control; P3: Group 3 With Control; P4: Group 4 With Control
Relevance
As is known, diabetic foot syndrome (DFS) and diabetic nephropathy are a consequence of the development of type 2 diabetes mellitus (type 2 diabetes) and are characterized by high morbidity and mortality among these patients [1.2]. At the same time, in patients with type 2 diabetes, the lifetime risk of developing a foot ulcer is 12–25% [one], while the risk of developing diabetic nephropathy is approximately 20-30% [2]. In dialysis patients, the risk of limb amputation is about 10 times higher than in patients with type 2 diabetes in general [3]. Some studies show that up to 10% of patients with type 2 diabetes have limb amputations when enrolled in a chronic dialysis program [4]. According to research, the pathogenesis of diabetic foot in end-stage renal disease is certainly multiple. However, US registry data on kidney disease suggest that prior diagnosis of peripheral vascular disease, elevated serum phosphorus, and mean systolic blood pressure are predictors of amputation within 2 years in dialysis patients [5]. But, despite the relevance of this topic, unfortunately, there is little data in the literature on a possible correlation between diabetic foot complications and renal failure in pre-dialysis patients with type 2 diabetes. Despite a recent study, data on more than 900,000 people collected by the UK Health Information Network revealed a strong association between CKD stages and diabetic foot ulcers [6]. But these results are difficult to interpret due to non-standardized definitions and methods for examining SDS between local institutions. Back in 2009Gunter Wolf noted that little is known about the potential association between renal function and the development of DFS in patients with preterminal renal failure [7].
Thus, the low life expectancy of patients with diabetic nephropathy with end-stage renal disease (ESRD) on dialysis is primarily due to the high incidence of other serious complications of diabetes. One of the complications that determine the high risk of disability and mortality in patients with type 2 diabetes with ESRD on dialysis is DFS. According to the authors [8-11], in patients with DM with the onset of ESRD (uremia), the risk of DFS increases by more than five times. With the initiation of renal replacement therapy, the frequency of DFS increases significantly [12-14]. At the same time, DFS not only significantly reduces the quality of life of patients, reduces the chances of a successful kidney transplantation, but also creates a real threat of limb amputation and a high risk of mortality. Based on our analysis of the literature, we concluded that after the start of renal replacement therapy in patients on hemodialysis, there is an increase in the incidence of neuroischemic form of DFS. Along with this, the progression of chronic obliterating diseases of the arteries of the lower extremities during the observation period was noted only among patients’ diabetes mellitus on hemodialysis. Therefore, it is necessary to find ways for early prevention of these complications, early diagnosis and treatment. All of the above emphasizes the relevance of the topic and was the reason for this study. Purpose of the study: explore state of renal function in patients with severe complications of diabetic foot syndrome (ulcer, gangrene, amputation) associated with chronic kidney disease.
Research Material
91 patients (prospectively) with type 2 diabetes were examined in the period 2021-2022 at the RSSPMC of Endocrinology, in the department of diabetic foot. All observed patients were divided into 4 groups:
a) 1 gr. – 25 patients with DFS complicated by ulcer, gangrene and amputation and in combination with CKD 4-5 stages on hemodialysis
b) 2 gr. – 25 patients with DFS complicated by ulcer, gangrene and amputation in combination with CKD stages 4-5 without hemodialysis
c) 3 gr - 20 patients with DFS complicated by gangrene and amputation without CKD.
d) 4 gr - 21 patients with DFS, without severe complications, with the initial stage of CKD.
The control group consisted of 20 patients with DM 2 without complications. To characterize the examined patients were used: general clinical, biochemical and instrumental examinations.
Research Methods
Biochemical (bilirubin, direct, indirect, lipid spectrum, ALT, AST, PTI, coagulogram, blood sugar, glycated hemoglobin, urea, creatinine, GFR, wound pathogens, procalcitonin, interleukin-6, vascular endothelial growth factorVEGF-A and instrumental: ECG, MRI of the feet, Dopplerography of the main vessels of the legs, ultrasound of the internal organs, the fundus. Secondary efficacy measures included blood glucose, blood lipids, wound area, lower extremity blood vessel diameter, blood flow rate, walking speed, etc.
Results of the Study and their Discussion
Table 1 shows the distribution of patients by sex and age. Thus, out of 91 patients, the majority were patients from 45 to 74 years old. There were 60 patients (65.9%) from 45 to 59 years old and only 21 patients (23.1%) over 60 years old. As can be seen from Table 1, the number of men dominated in all groups of patients. Our next step was to perform a comparative analysis of biochemical parameters by groups Table 2. As can be seen from Table 2, the highest rates of fasting glycemia were observed in patients of group 2, that is, with DFS and CKD 4-5 stages without hemodialysis. Significantly lower hemoglobin values were also observed in this group of patients (p<0.001), glycated hemoglobin significantly higher values of urea, creatinine and GFR (p<0.001). All patients had significantly reduced values of HDL (p<0.001) and total cholesterol (p<0.05). Russian author Bublik E.A. in 2008 showed in her work that the progression of chronic obliterating diseases of the arteries of the lower extremities during the observation period was noted only among patients with type 2 diabetes on hemodialysis. During the hemodialysis procedure, there is a decrease in systolic blood pressure, both in the arteries of the shoulder, and in the arteries of the legs and first toes, which can lead to a deterioration in the blood supply to the lower extremities and contribute to an increase in the risk of neuro-ischemic form of the diabetic foot syndrome [15].
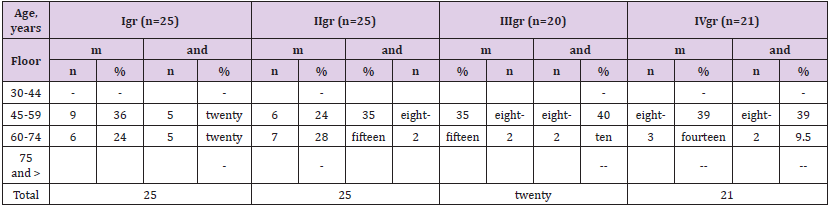
Table 1: Distribution of patients by age, sex and groups (according to WHO).
Note: M - number of men, W - number of women
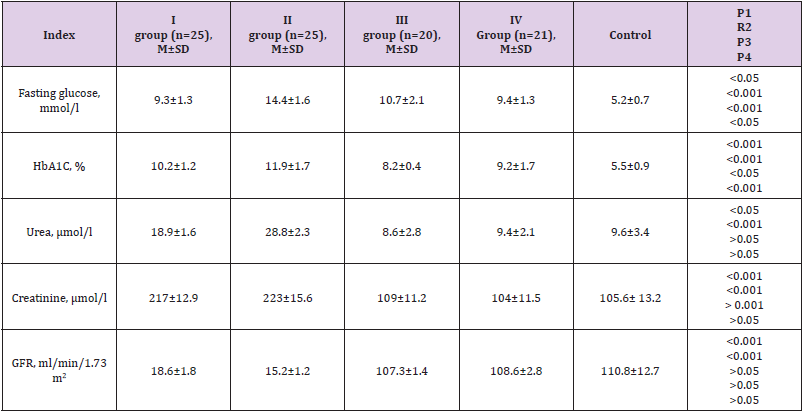
Table 2: Average biochemical blood parameters of patients by groups.
Note: AH: Arterial Hypertension; DBP: Diastolic Blood Pressure; SBP: Systolic Blood Pressure; p: Reliability Criterion
The data of the performed literature review led to the conclusion that this direction is very relevant. However, there are no randomized placebo-controlled trials in patients with type 2 diabetes subjected to a thorough study of the pathogenesis of the progression of two competing severe complications of the disease - DFS and CKD. Important indicators of the functional state of the kidneys are the data of the general analysis of urine Table 3. A wellknown criterion for proteinuria is also the albumin-creatinine ratio (A/Cr). As can be seen from Table 3, this ratio was significantly increased in groups 1 and 2 of patients. (p<0.01, p<0.001.). The levels of albuminuria were also significantly high in the groups of patients (p<0.01, p<0.001.), while the density of urine was significantly below the norm in all groups of patients. (p<0.01). The results of our studies showed that in patients with DM 2 with DFS and CKD on hemodialysis, the worst indicators of biochemical studies were revealed compared with other groups of patients.
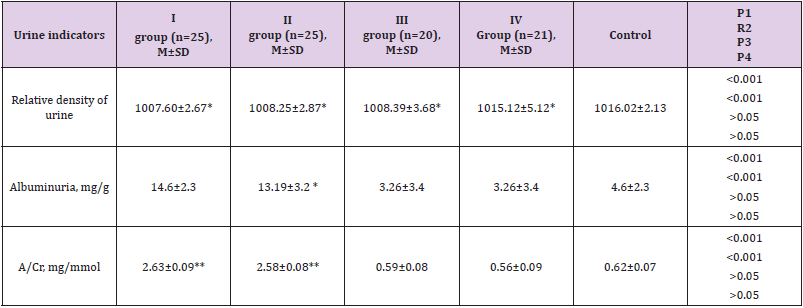
Table 3: Average biochemical blood parameters of patients by groups.
Note: * - significance of differences between patients with DM and control, one sign * p<0.05, two signs ** - p<0.01, three signs *** - p<0.001, while p1 is the significance of differences between group 1 and control, p2 - group 2 with control, p3 - group 3 with control, p4 - group 4 with control
Conclusion
Biochemical parameters were significantly impaired in patients of group 1, that is, with DFS and CKD 4-5 stages on hemodialysis, which indicates the need for further research in this group of patients.
References
- Sing N, Armstrong DG, Lipsky BA (2005) Preventing foot ulcers in patients with diabetes. JAMA 293(2): 217-228.
- Ritz E, Orth SR (1999) Nephropathy in patients with type 2 diabetes mellitus. N Engl J Med 341(15): 1127-1133.
- Schomig M, Ritz E, Standl E (2000) The diabetic foot in the dialyzed patient. J Am Soc Nephrol 11(6): 1153-1159.
- Papanas N, Liakopoulos V, Maltezos E (2007) The diabetic foot in end stage renal disease. Ren Fail 29(5): 519-528.
- O Hare AM, Bachetti P, Segal M (2003) Factors associated with future amputations among patients undergoing hemodialysis: results from the dialysis morbidity and mortality study waves 3 and 4. Am J Kidney Dis 41(1): 162-170.
- Margolis DJ, Hofstad O, Feldman HI (2008) Association between renal failure and foot ulcer of lower-extremity amputation in patients with diabetes. Diabetes Care 31(7): 1331-1336.
- Gunter wolf, Nicolle Muller, Martin Busch, Gudrun Eidner, Christoph Kloos, et al. (2009) Diabetic foot syndrome and renal function in type 1 and 2 diabetes mellitus show close association Nephrology Dialysis Transplantation 24(6): 1896-1901.
- Eeight Kalashnikova MF, Maksimova NV, Udovichenko OV, Suntsov YuI (2010) Pharmacoeconomic aspects of the treatment of diabetic foot syndrome. Diabetes mellitus (2): 113-119.
- Urmanova Yu M, Kholikov A Yu (2013) Changes in the nervous system in patients with type 2 diabetes mellitus with nephropathy and the prognostic significance of neuromarkers of brain damage. Literature review. Eurasian Union of Scientists. Series: medical, biological and chemical sciences 8(89): 3-8.
- Maksimova NV (2011) Clinical and economic analysis of conservative tactics in the treatment of patients with diabetic foot syndrome in Moscow. Diss. PhD Moscow.
- Maslova OV, Suntsov YuI (2011) Epidemiology of diabetes mellitus and microvascular complications. Diabetes mellitus 3: 6-9.
- Risman, Boris Veniaminovich (2011) Treatment of purulent-necrotic complications of diabetic foot syndrome. Diss. MD St. Petersburg.
- Sadovoy MA (2005) Ensuring the quality of medical care based on international standards ISO 9000. Chief Physician 5S: 36-41.
- Hinnen DA, Buskirk A, Lyden M, Amstutz L, Hunter T, et al. (2015) Use of Diabetes Data Management Software Reports by Health Care Providers, Patients with Diabetes, and Caregivers Improves Accuracy and Efficiency of Data Analysis and Interpretation Compared with Traditional Logbook Data: First Results of the Accu-Chek Connect Reports Utility and Efficiency Study (ACCRUES). Journal of Diabetes Science and Technology. Mar 9(2): 293-301.
- Bublik E A (2008) Lesions of the lower extremities in patients with diabetes mellitus with end-stage chronic renal failure// diss on soisk. uch. Art. PhD according to special 14.00.03 - Endocrinology, Higher Attestation Commission of the Russian Federation 133.
