 Research Article
Research ArticleABSTRACT
Introduction: Gestational diabetes is the most frequent endocrine disease of pregnancy and generally appears when there are risk factors.
Objective: To describe the clinical epidemiological behavior of Gestational Diabetes in the Orlando Matos Mosqueda polyclinic in the period 2019-2021.
Methods: A descriptive and cross-sectional study was carried out on a universe of 57 patients with gestational diabetes in the aforementioned health area, the universe coincided with the sample. The data sources were collected from the attendance of the patients to their consultations, the field visits; of clinical histories and family files, using a survey to collect said information. Descriptive statistics techniques were used to generate the distributions of absolute frequencies and percentages.
Results: 31.58% of the patients belonged to the age group 35-39 years, 43.86% had a BMI of 30-34.9. 96.4% had a risk factor, 55.56% had a history of a BMI prepregnancy greater than 25kg/m2. The most frequent maternal complications were vaginal infections (50.88%) and urinary infections (21.05%). While the macrofetus (33.33%) the fetal complication that prevailed.
Conclusion: The predominant age group was 35-39 years and the BMI was 30- 34.9 Kg/m2. The risk factor pregestational BMI greater than 25kg/m2 was the most frequent. The maternal complications that predominated were vaginal and urinary infections, and in fetal complications, macrostomia and prematurity.
Keywords: Gestational Diabetes; Risk Factors; Primary Health Care
Introduction
Pregnancy is a physiological process that, with a certain frequency (20%), can suffer various alterations, among which are genetic alterations and malformations of the fetus, preterm birth, preeclampsia and placental insufficiency, endocrine-metabolic disorders such as diabetes gestational (GD) and nutritional disorders. That is why the medical community adopted a series of procedures (care and observations) that allow preventing or diagnosing these alterations early. Gestational diabetes is defined as a hydrocarbon intolerance of variable intensity, with onset or first recognition during pregnancy, regardless of the treatment used for its control and its postpartum evolution [1,2]. The new diagnostic strategy for GD is much simpler and proposes a universal screening, so that in the first prenatal assessment, blood glucose should be determined baseline, glycosylated hemoglobin or casual blood glucose (without prior fasting) to detect undiagnosed diabetes early and start treatment in the same way as it is done with diabetic pregnant women prior to pregnancy. Thus, diabetes is diagnosed if any of the following criteria are met: (1), random blood glucose greater than 11 mmol/L (200mg/dl) with classic symptoms of diabetes, fasting blood glucose 7 mmol/L (125Mg/dl ) on 2 or more occasions, PTG greater than 11mmol/l (200mg/dl) at 2 hours. In clinical practice, the coincidence of diabetes and pregnancy occurs in two different circumstances: gestational diabetes and pregestational diabetes. 0.3% of women of childbearing age are diabetic while between 0.2 and 0.3% of all pregnancies, the woman has diabetes prior to gestation.
Gestational diabetes causes complications in 1 to 4% of pregnancies [3]. During pregnancy, a series of changes occur in glucose metabolism that seek to meet the needs of the fetus: reduction of fasting blood glucose and acceleration of biochemical reactions in the fasting phase is what is known as “ accelerated fasting”, reduced insulin sensitivity, which manifests itself in the second half of pregnancy and causes an increase in the secretion of said hormone [4]. Fetal glucose consumption and decreased hepatic gluconeogenesis due to lack of substrate, are the mechanisms involved in “accelerated fasting”, while the factors that condition insulin resistance are related to the action of different hormones and cytokines that are elevated during pregnancy (placental lactogen, prolactin, progesterone , cortisol, estradiol, placental tumor necrosis factor α (TNF-α) and free fatty acids) [5]. During the first trimester of pregnancy and the early stages of the second, insulin sensitivity is increased due to higher concentrations of circulating estrogens, causing an expansion of adipose tissue together with an increase in energy stores, especially all of the adipose tissue; but it is from weeks 24 to 28 of gestation, when a gradual increase in insulin resistance occurs, which can reach the levels observed in patients with type 2 diabetes mellitus. This resistance of hormonal origin in women pregnant, seems to be due to a combined effect between the increase in adipose tissue and the effects of various substances produced by the placenta [6].
The clinical importance of gestational diabetes lies in the morbidity and mortality maternal and fetal, although complications can be reduced after applying the appropriate treatment. Thus, in the study entitled “Australian Carbohydrate Intolerance Study in Pregnant Women” (ACHOIS) it was shown that the incidence of serious perinatal complications was 4% in the 510 women with gestational diabetes in the study who were not treated, while the incidence of serious perinatal complications was only 1% in the 490 women with gestational diabetes undergoing dietary and/or pharmacological treatment. According to this study, the minimum number of women who need treatment to avoid a serious perinatal event is 34 women. This indicates that serious perinatal complications occur in 3% of undiagnosed or untreated cases of gestational diabetes [7]. The 2016 WHO-PAHO report on hyperglycemia and pregnancy states that it affects between 1% and 35% of pregnant women globally. Estimates for the Americas region indicate that hyperglycemia may be present in between 11% and 12% of pregnancies (adjusted prevalence of 11.9% and 11.5% in the North America-Caribbean and South-Central America subregions, respectively), where the disease can be found in 85% of cases.
The prevalence of GD in the United States is between 1% and 14%, depending on the population studied as well as the diagnostic criteria used. In Mexico it is estimated that it is 4.3%, in Argentina from 5 to 8% and in Spain 12%. There are ethnic groups in which the frequency is very low, such as in the populations of Taiwan (0.7%), while in others it is very high, as is the case of the Zuni Indians [8]. Studies on DG in Cuba have reported that it is approximately 4.5%, so there is no great difference with what is found in the rest of the world [9]. Primary Health Care is medical care aimed at solving the specific health needs and problems of each community, which must be addressed through coordinated activities of promotion, prevention, diagnosis, treatment and rehabilitation, and at the same time to promote the self-responsibility of the individual and the community with their active participation. It includes a set of procedures and services, as well as the protection of specific population groups and the care of health problems with the appropriate analytically directed technologies. Being the first level of contact of the National Health System (SNS) with the people, the family and the community, it can be ensured that it is the indicated one to apply the prevention and diagnosis measures of the disease.
The DG within the Havana province, in the Arroyo Naranjo municipality no studies have been reported that provide up-to-date information on the subject; particularly the doctors and nurses who care for the population belonging to the Orlando Matos Mosqueda Polyclinic do not have a clinical epidemiological characterization of patients with GD, which makes it difficult for them to manage pregnant women from their condition, and, logically, prevention and diagnosis early disease; hence the need to carry out the proposed research, based on the following scientific problem: The results of the study made it possible to identify the main risk factors to prevent and adequately manage GD from the primary care level, as well as to systematize promotional behavior in doctors and nurses without the use of complex and expensive technologies or a high consumption of time and resources.
Methods
An observational, descriptive and cross-sectional study was carried out on 57 pregnant women from the Orlando Matos Mosqueda polyclinic, located in the Arroyo Naranjo municipality, during the period from January 2019 to December 2021. The main data sources used were collected from the attendance of the patients to their respective consultations and the visits that were made to their homes to observe, question and examine them; in addition to the data that was collected in the medical records and family records, using a survey to collect said information.
Inclusion criteria.
• Being pregnant, with a diagnosis of Gestational Diabetes.
• Belong to the Orlando Matos Mosqueda polyclinic.
The universe was made up of 57 patients diagnosed with gestational diabetes at the Orlando Matos Mosqueda polyclinic during the period from January 2019 to December 2021. The sample coincided with the universe. The variables used were maternal age, nutritional assessment, maternal risk factors for gestational diabetes, maternal and fetal complications. Descriptive statistics techniques were used to generate the distributions of absolute frequencies and percentages, for all the variables; Statistical arithmetic mean, minimum, maximum and standard deviation were calculated to summarize the information corresponding to age. To determine if there is an association between the qualitative variables of interest for the study, the Pearson Chi-square statistical test was used with a significance level of 5%. The results were presented in tables and graphs for better understanding. The research was carried out with due respect for the integrity of the people, their autonomy and anonymity, using the informed consent of the patient to have her authorization to participate in the study. All people were treated equally, regardless of their physical condition, sex, age, race, and economic or cultural level.
Results
Source: Clinical Records. As shown in the Table 1 above, the vast majority of patients diagnosed with gestational diabetes are between the ages of 35-39 years (31.58%), with almost half of the patients studied being in this age range. Source : Clinical Records, BMI : IBody Mass index : Kg/m2. The Table 2 above shows how most of the patients studied are obese and overweight; 46 patients with a BMI greater than 25Kg/m2 were found, which represents 80.70% of the total number of patients studied, 25 of them have a BMI between 30-34.9 Kg/which represents 43.86% of the total and 17 (29.82 %) with a BMI between 25-29.9 Kg/m2. A lower number is observed among patients with a BMI of 18.6-24.9 Kg/m2, only 9 patients (5.79%) and those with a BMI less than 18 Kg/m2, with only 2 representing 3.51%. Source: Information obtained from medical records. N : 57 Note: In some cases there is the possibility that the same patient has 2 or more risk factors. It can be seen in the previous Table 3 how there is a greater number of patients in whom some risk factor is present to develop the disease, represented by a total of 54 patients for 96.40%, and only 3 without any risk factor, representing only the 3.6%. The predominant maternal risk factor was pregestational BMI greater than 25Kg/m2 (55.56%) followed by maternal age greater than 35 years, which is present in 38.89% of the patients. Source: Information obtained from medical records N= 57. Note: In some cases there is the possibility of the existence of two or more maternal complications. As shown in the previous Table 4, vaginal infections predominate during pregnancy in these patients in 50.88%, followed by urinary infection that occurred in 21.05% of cases, while hypertensive disorder in 15.79%, the premature delivery in 10.53% of the cases, the rest did not obtain significant figures. Source : Information obtained from medical records. N : 57 Note: In some cases there is the possibility of the existence of two or more fetal complications in the same patient. As shown in the Table 5, the most frequent fetal complication was macrosomia with 19 newborns in this condition, which represented 33.33% of the cases, followed by premature and low birth weight, which were reported with equal figures. (10.53%).
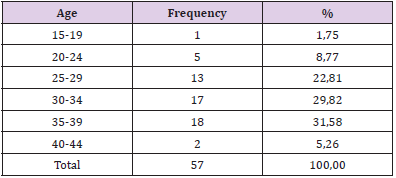
Table 1: Patients with gestational diabetes according to age.
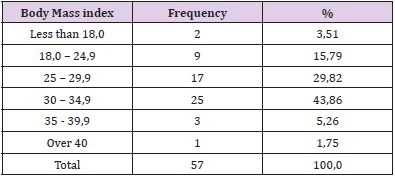
Table 2: Nutricional assessment by body mass index.

Table 3: Maternal Risk Factors.
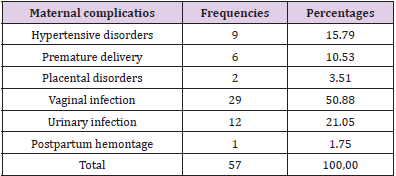
Table 4: Maternal Complications.
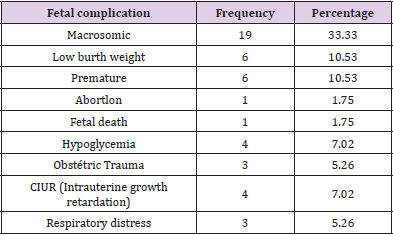
Table 5: Fetal complications.
Discussion
In Cuba, the diagnosis of Gestational Diabetes is a prioritized problem in the National Maternal and Child Program, this is carried out from the first prenatal control in Primary Health Care (PHC), hence the margin of error in its diagnosis is insignificant according to the authors’ criteria. In Cuba, the National Program for the Care of Pregnant Women with Diabetes was established, currently included in the Maternal and Child Care Program and associated with the National Diabetes Program, where it is established that late identification, delayed referral and births occurring should be avoided. in institutions not prepared to handle these cases, since all this can be associated with poor maternal and perinatal outcomes. Taking this into account is what has made it possible to reduce the usual complications in diabetic pregnant women [9]. In Cuba, the diagnosis is made taking into account the WHO criteria and fasting blood glucose is used for this. A fasting blood glucose level during pregnancy is considered to be one with a value between 4.4 mmol/L - 5.5 mmol/L or more. When these blood glucose figures appear in a pregnant woman, a 2-hour glucose tolerance test (GTT) should be indicated and 75 g of glucose administered to determine whether or not the disease exists [9]. The search for Gestational Diabetes has great epidemiological importance due to the fact that a good control of the metabolism significantly reduces the risk of maternal-fetal complications and allows early detection of a population of women at risk of contracting diabetes mellitus after the end of pregnancy, for which it is a priority in the program Maternal Child in Cuba.
One of the risk factors with the greatest weight in the development of GDM is age 30 years or older, since it is associated with insulin resistance. In the present investigation, the predominance of the age group of 35-39 years is reported, differing from those obtained by Paredes Quintero, PP [10] who reported ages between 26-30 years. We also disagree with the results, in Chile, where Huidobro, et al. [11] found that the age was 25.9 ± 7.0 years. Santana M, et al. [12] reported ages of 35 years with a SD ± 3.5 with similar results to the present study. Research carried out in Cuba by Abreu C, Santana T, Mánchola E, Viamontes A and others [13] report ages between 20 and 40 years for 97% and Cruz J, Pérez A, Yanes M, Hernández P, [14] report that the mean age was 29.2 ± 5.3 years, a range that does not cover the predominant group in this research. Márquez A, Valdés L, Lang J, Cruz J, Piloto M, Iglesias I, et al. [15] report that the mean age in patients with GDM exceeds 30 years, coinciding with this study, so the authors reinforce the importance to take into account the age of 30 years and over to develop Gestational Diabetes. Overweight and obesity in pregnant women are a health problem and are a constant concern; in primary health care where actions can be taken to prevent these diseases, which are also risk factors for high blood pressure in pregnancy.
When there is obesity or overweight, the risk of suffering from gestational diabetes increases from two to six times more, compared to pregnant women of normal weight. Jeddú Cruz Hernández, Arisleydis Pérez Fundora, Marelys Yanes Quesada, Pilar Hernández García [14] conducted a study that included 242 women with gestational diabetes, treated at the “América Arias” Gynecobstetric Hospital in Havana, reporting excessive pregestational weight in one (51 .71%) coinciding with this study. Like Yerani Ferrer-Martín Y, García-Pérez RP, Rodríguez-DuménigoR [16]. who investigated the prevalence of risk factors for gestational diabetes in the obstetric population of Ciego de Ávila made up of 2,200 pregnant women in 2018, reporting obesity as an important factor in GDM. The majority of pregnant women with gestational diabetes presented some type of . risk factor and of them the pregestational BMI of more than 25kg/m2 and age over 35 years were, in that order, the most frequent. In a case-control study in Mexican pregnant women, maternal age over 35 years was identified as a risk factor, as in our study [17]. Obesity was also a risk factor found in a study in Santiago de Cuba, however the largest number of pregnant women were not over 30 years of age, which does not coincide with our research [18]. For his part, Cajigal, [19] in a study in Ciego de Avila found that obesity was also a risk factor associated with gestational diabetes, although in a smaller number of pregnant women than in ours. Vaginal and urinary infections, hypertensive disorders and premature birth appear as the most frequent complications in pregnant women under study.
Bustamante [20] exposes how the high level of glucose in the blood can put the mother and her unborn child at risk and affirms that all those affected must have strict hospital control regarding gestational diabetes. An investigation showed that 13% of pregnant women with gestational diabetes presented hypertensive disorders as maternal complications and half presented urinary tract infections, [21] in our study the results were similar in hypertensive disorders, not being so in urinary infections that occurred in fewer patients. In Cuba, the authors agree that women with gestational diabetes are at risk of complications. Fernández [22] reports preeclampsia and a high risk of intrauterine growth restriction and postpartum chronic arterial hypertension as the most frequent maternal complications, and the Cuban Program for Comprehensive Care of Pregnant Women with Diabetes Mellitus [23] exposes 12% of preterm deliveries coinciding with with our study and 5% of preeclampsia as maternal complications. The most frequent fetal complications in our study were macrosomic newborns, low birth weight newborns and preterm births. In a similar study, Quintero [24] found macrosomia in 18.6% and in ours it reached 33.3%. Neonatal hypoglycemia and low birth weight and prematurity largely coincided with our results. For their part, Rodríguez, et al. [25] posit prematurity in 17.4%, low birth weight in 13.1, and macrosomia in 15.3% of the cases studied, coinciding with the leading causes of complications. fetal gestational diabetes. Gestational diabetes is the most frequent metabolic complication of pregnancy, being considered a heterogeneous and complex pathology that involves the maternal biological system, the placental tissue and the fetus [26,27].
Conclusion
The predominant age group was 35-39 years and BMI 30- 34.9 Kg/m2. The risk factor BMI (Body Mass Index) pre-pregnancy greater than 25kg/m2 was the most frequent. The maternal complications that prevailed were vaginal and urinary infections, and in fetal complications, macrosomia and prematurity.
Authors Contribution
• Pedro Rolando Lopez Rodríguez: He reviewed clinical histories and searched for bibliography. He chose the sampling method selecting the study population and analyzed and discussed the table content. He drafted the document.
• Rene Jorge Mena Mujica: Helped in the review of medical records and search Bibliography, performed statistical processing, calculated arithmetic mean and standard deviation of quantitative variables.
• Ana Ivis Estrada Casteleiro: Performed the statistical processing, calculated and she interpreted the chi-square and associated variables according to Duncan’s docima.
• Elisa Maria Puentes Rizo: She reviewed the literature on the subject looking for data worldwide epidemiological data, designed the study methodology, classified the research, processed the information and limited the bibliographical references according to Vancouver standards.
References
- (2014) American Diabetes Association. Standards of Medical Care in Diabetes 2014. Diabetes Care 37 (Suppl 1): S14-S80.
- Moyer VA (2019) Screening for Gestational diabetes Mellitus: U. S. Preventive Services Task Force Recommendation Statement. Ann InternMed 160(6): 414-420.
- Jafari Shobeiri M, Ghojazadeh M, Azami Aghdash S, Naghavi Behzad M, Piri R, et al. (2015) Prevalence and Risk Factors of Gestational Diabetes in Iran: A Systematic Review and Meta-Analysis. Iran J Public Health 44(8): 1036-1044.
- Huillca Briceño A, Romani Varillas M (2019) La multiparidad como factor de riesgo de diabetes mellitus gestacional. Revista cubana de obstetricia y ginecología 42(2).
- Garcia C (2018) Diabetes mellitus gestacional. Med Int Mex 24: 148-156.
- De Leiva A, Mauricio D, Corcoy R (2007) Diabetes-Related Autoantibodies and Gestational Diabetes. Diabetes Care 30: S127-133.
- Spong CY, Thom E, Carpenter MW, Ramin SM (2015) A multicenter, randomized trial of treatment for mild gestational diabetes. N Engl J Med 367(14): 1633-1639.
- (2015) Hiperglicemia y embarazo en las Amé Informe final de la ConferenciaPanamericanasobre Diabetes y Embarazo. Lima (Perú), 8-10 de septiembre del 2015. Organización Panamericana de la Salud 74: 65-69.
- (2019) Dirección Provincial de Salud de La Habana. Registro Estadístico Primario 2015-2019. La Habana.
- Paredes Quintero PP (2022) Factores de riesgo asociados a la diabetes mellitus. Revista Cubana de Medicina General Integral 38(1): e1440.
- Huidobro A, Torres D, Paredes F (2017) Diabetes Gestacional: asociación con grupo ABO. Rev méd Chile 145(4).
- Santana M, Esquivel M, Herrera V, Castro B, Machado M, et al. (2020) Atención a la salud materno-infantil en Cuba: logros y desafí RevPanam Salud Pública 42(27).
- Abreu C, Santana T, Mánchola E, Viamontes A (2017) Caracterización clínica de la diabetes gestacional en el Policlínico Ignacio Agramonte de 2011-2015. RevArchMed Camagüey 21(6).
- Cruz J, Pérez A, Yanes M, Hernández P (2020) Factores de riesgo de diabetes gestacional en mujeres embarazadas de una maternidad de La Habana. Rev Cuba de Med Gen Integr 36(2).
- Márquez A, Valdés L, Lang J, Cruz J, Piloto M, et al. (2018) Segundo Consenso Cubano de Diabetes y Embarazo. Rev Cubana Endocrinol 29(1).
- Yerani Ferrer Martín Y, García Pérez RP, Rodríguez Duménigo R (2021) Prevalencia de los factores de riesgo de la diabetes gestacional en la población obstétrica de Ciego de Á Revista Médica Electrónica de Ciego de Ávila 27(1): e1782.
- Domínguez Vigo P, Álvarez Silvares E, Alves Pérez MT, Domínguez Sánchez J, González A (2016) Incidencia y factores clínicos de riesgo de diabetes mellitus en mujeres con diabetes gestacional previa. Ginecol obstet Méx 84(4): 228-242.
- Casas Lay Y, Sánchez Salcedo M, Álvarez Rodríguez JM (2014) Algunas variables epidemiológicas en pacientes con diabetes mellitus gestacional. Rev Cubana Obstet Ginecol 40(1): 2-12.
- Cajigal Pelegrín Y, Rodríguez LA (2015) Algunas variables relacionadas con el diagnóstico de la diabetes gestacional en Ciego de Á MediCiego 21(3): 27-33.
- Bustamante A (2019) Relación entre diabetes gestacional y hemorragia postparto. Hospital II –2 Tarapoto. Trujillo: Universidad César Vallejo.
- Yagual Cochea, Karen Estefanía (2022) Factores de riesgo obstétrico y su influencia en complicaciones maternas. Centro de salud San Antonio. 2021. La Libertad. UPSE, Matriz. Facultad de Ciencias Sociales y de la Salud, p. 77.
- Fernández C, Luna M, Lorenzo M, Magaz A, Beceiro L (2016) Importancia de la detección de factores de riesgo para diabetes mellitus gestacional. Index Enferm 25(1-2).
- Márquez A (2015) Programa Cubano de Atención Integral a la Gestante con Diabetes Mellitus. Conferencia Panamericana de Diabetes y Embarazo, Lima, Perú
- Quintero Paredes P (2022) Factores de riesgo asociados a la diabetes mellitus gestacional. Revista Cubana de Medicina General Integral 38(1).
- Rodríguez J, Díaz Agüero H, Amador de Varona CI, Valdés Dacal S (2014) Tratamiento de la diabetes mellitus en el embarazo. Arch Med Camag 18(4).
- Rodríguez Fernández JM, Díaz Agüero H, Amador de Varona CI, Ignacio Cabrera Figueredo, Plácido Luaces Sánchez, et al. (2020) Caracterización materna-perinatal de las gestantes diabé AMC 21(1).
- Mitanchez D (2018) Recién nacido de madre diabé EMC – Pediatría 53(3): 1-13.
