 Research Article
Research ArticleAbstract
This study aimed to estimate the optimal clamping force of ultra-high-molecularweight polyethylene (UHMWPE) cables based on contact pressure distributions indicating blood flow by focusing on the mechanical factor of contact pressure. UHMWPE cables with widths of 3 mm and 5 mm were used. A pressure sensor was set on an artificial femur, and the cables were wrapped on simulated tissues and tightened with clamping forces of 10, 20, and 30 kgf based on the indication values displayed on the tightening guns. Removal of the tensioner after clamping was defined as release, and the contact pressure with each clamping force was measured. After the cable with a width of 3 mm was clamped with a force of 10 kgf and released, the contact area was 31.2 mm2; the ratio of the contact area to the entire surface of the cable was calculated, which showed that approximately 30% made local contact. The ratio did not change significantly and remained at 30% even when the clamping force increased to 15 kgf. After the cable with a width of 5 mm was clamped with a force of 10 kgf and released, the contact area ratio was approximately 40% and it remained the same as the clamping force increased to 15 kgf. Blood flow disorders can be avoided with UHMWPE cables fixed under clamping forces of 10 kgf and 15 kgf. Considering the conservation of the fixing force, the optimal clamping force of UHMWPE cables is determined to be 15 kgf.
Keywords: Osteosynthesis; Cerclage Cable; UHMWPE Cable; Optimal Clamping Force; Contact Pressure
Introduction
Cerclage cables used in osteosynthesis should be discussed from the mechanical aspect of maintaining the fixing force at fracture sites and from the biological aspect of maintaining unobstructed blood flow. It is important to examine the optimal clamping force for achieving stable clamping, and the presentation of such data from both perspectives will help surgeons in the use of cerclage cables. Although many biomechanical studies on metal cables have been conducted, only a few cases involving the use of UHMWPE cables have been reported [1-3]. The string shape and tape-like braided shape of UHMWPE cables were developed in 1988 and 2000, respectively [4,5]. UHMWPE cables were initially used mainly in spinal surgeries such as scoliosis correction [6-8]. UHMWPE cables have also been used in osteosynthesis for trauma since 2010 and in surgeries for subtrochanteric fractures, fractures around artificial hip stems (Figure 1a), fractures of the lateral malleolus, distal interphalangeal joint arthrodesis, and other surgeries [9-11]. UHMWPE cables exhibit more favorable biomechanical performance than metal cables [12]. Although UHMWPE cables are expected to feature favorable mechanical performance, a case of poor blood circulation was reported; this was attributed to the flexibility by which UHMWPE cables are characterized [13]. Blood flow is obstructed by UHMWPE cables because the cables remain tightened even after release, which presents issues pertaining to solid fixation and unobstructed blood flow. Judging from both the biological and the mechanical aspects, we estimate that the optimal clamping force will be lower than that expected by surgeons. Main arteries around the femoral diaphysis include the superficial femoral artery and the deep femoral artery. It has been pointed out that clamping may obstruct these arteries or the periosteal artery [14]. Thus, in this study, we judged whether blood could flow based on contact pressure distributions and used the contact area ratio as an index. This study aimed to estimate the appropriate clamping force for UHMWPE cables by focusing on a mechanical factor of contact pressure for judging fixing forces.
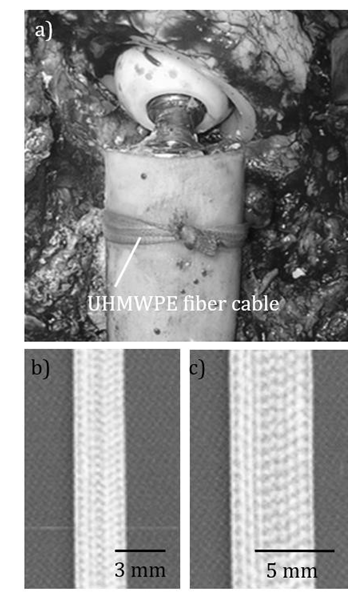
Figure 1: UHMWPE cables.
a) Cable used in revision total hip arthroplasty.
b) 3-mm-wide cable.
c) 5-mm-wide cable.
Materials and Methods
This study did not involve humans and did not require IRB approval. We studied UHMWPE cables (NESPLON® cable system, Alfresa Pharma Corporation, Japan) with widths of 3 mm and 5 mm (Figures 1b & 1c). We used a femur simulating the human anatomical shape (Sawbones #3403, Pacific Research Laboratories, Inc., WA, USA) for clamping each cable on the femoral diaphysis. During osteosynthesis, tissues can remain unremoved depending on the fracture sites and procedures. Sus scrofa domesticus thigh tissues with thicknesses of 2 mm and 5 mm were prepared for simulating tissues [15]. Based on the assumption of a fracture around a hip stem, a thin pressure sensor (Surface pressure distribution measurement system I-SCAN, NITTA Corporation, Japan) was set on the femoral diaphysis, and the cables were wrapped on the tissues and tightened with a fastener of each cable (Figure 2). This system detects contact pressures of 0.1 MPa to 5.0 MPa with the conductive ink set at the sensor site that is 50 mm in length, 50 mm in width, and 0.1 mm in thickness.
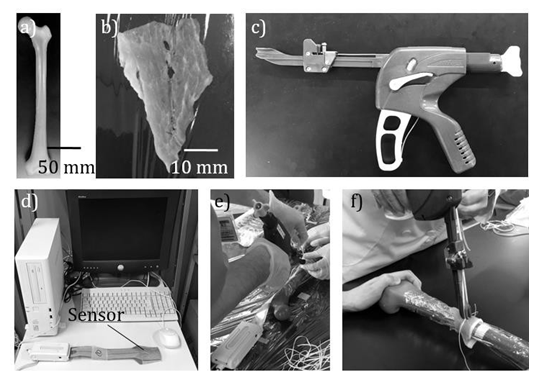
Figure 2: Materials and systems.
a) Artificial femur.
b) Sus scrofa domesticus thigh tissue (thickness:2 mm or 5 mm).
c) A tensioner of UHMWPE cables (Tightening gun).
d) Pressure distribution analysis system.
e) UHMWPE cables wrapped around tissue on diaphysis.
f) UHMWPE cables clamped by the tightening gun.
When pressure is applied on any of the 2000 sensing points, the electrical resistance changes. The pressure is converted to an 8-bit digital value and input into a personal computer. The UHMWPE cable was fastened using a knot and retightening using a tightening gun. Nodes were created by employing a double loop sliding knot, as performed in clinical practice, and tied down. This was followed by tensioning by adding one knot and finally fixing the attachment by adding another knot. The UHMWPE cables were gradually tightened under forces of 10, 20, and 30 kgf and fastened with the maximum value of the clamping force indicator, 30 kgf. A state with the tightening gun removed is regarded as released, under the assumption of being indwelled in the body, in clinical cases. The contact detection pressure and contact detection cell count were obtained from the contact pressure distribution, and the contact area was calculated based on the sensor area. As the contact pressure in the sleeve and knot of each cable increased, the clamping site was excluded from data processing. The optimal clamping force was estimated to range from 10 kgf to 20 kgf. Subsequently, the contact pressures under clamping forces of 10 kgf and 15 kgf were measured, and the contact area and contact area ratio were calculated.
Results
It was revealed that, under clamping forces of 20 kgf and 30 kgf, the entire surface of both cables with widths of 3 mm and 5 mm was used for contact with both tissues with thicknesses of 2 mm and 5 mm, which showed that the optimal clamping force was below 20 kgf. Furthermore, a comparison of the contact pressures under clamping forces of 10 kgf and 15 kgf showed that the contact pressure of the cable with a width of 3 mm and a clamping force of 10 kgf was equal to that with a clamping force of 15 kgf (Figure 3a). A significant difference was noted in the contact pressures of the cable with a width of 5 mm for clamping forces of 10 kgf and 15 kgf (Figure 3b). The contact pressure distributions under clamping forces of 10 kgf and 15 kgf showed that the pressures of both the cables were locally distributed and did not exhibit a distribution using the entire surface for contact, as obs erved for the clamping forces of 20 kgf and 30 kgf (Figures 4a & 4b). The tissue with a thickness of 2 mm was wrapped on the femoral diaphysis, and the cable with a width of 3 mm was clamped on the tissue with a force of 10 kgf and released.
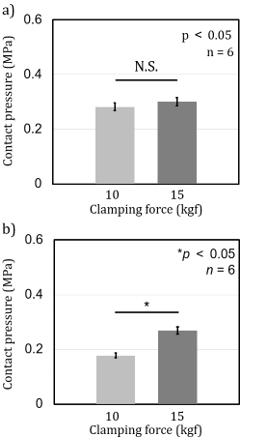
Figure 3: Contact pressure at each clamping force.
a) 3-mm-wide UHMWPE cable.
b) 5-mm-wide UHMWPE cable.
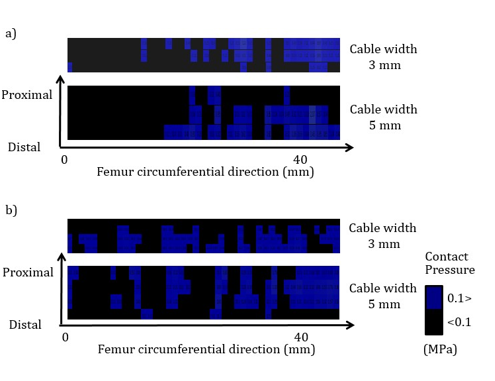
Figure 4: Contact pressure distribution.
a. Clamping force of 10 kgf after release.
b. Clamping forceof 15 kgf after release.
Subsequently, the contact area was 31.2 mm2 (Table 1). The ratio of this area to the entire surface of the cable was calculated to be 30.1±6.7%, which revealed that approximately 30% made local contact. The ratio remained essentially unchanged at 31.6±7.2%, with an increase in the clamping force to 15 kgf (Table 2). The tissue with a thickness of 2 mm was wrapped on the femoral diaphysis, and the cable with a width of 5 mm was clamped on the tissue with a force of 10 kgf and released. Thereafter, the contact area was 100.3 mm2. The ratio of this area to the entire surface of the cable was calculated to be 38.2±7.8%, which revealed that approximately 40% made local contact. The ratio remained essentially unchanged at 37.6±9.9%, with an increase in the clamping force to 15 kgf.

Table 1: Difference between maximum contact area and contact area after release for each tissue thickness and UHMWPE fiber cables with widths of 3 mm and 5 mm.

Table 2: Ratio of the contact area of contact pressure distribution to cable installation area.
Discussion
Tomita et al. reported that UHMWPE cables have excellent creep resistance and tension holding capacity through in vivo and in vitro experiments [16]. A study on animals showed that no macroscopic or histological abnormalities such as inflammation or fibrous tissue formation had been noted 16 weeks after the clamping of UHMWPE cables [17]. Jingushi, et al. concluded that UHMWPE cables were useful for the re-attachment of the osteotomized greater trochanter in hip surgery [11]. Although studies on materials, animals and clinical reports on UHMWPE cables have been noted, studies on the optimal clamping force in terms of blood flow are scarce. This study determined the optimal clamping force of a UHMWPE cable clamped on a femoral diaphysis under the assumption of a fracture around the artificial hip stem. It was confirmed that the clipping of residual soft tissues with thicknesses of 2 mm and 5 mm, using forceps when clamping, had no significant influence on the contact area, which suggested that the excessive removal of tissues was not required.
Blood vessel injuries associated with tissue removal and blood flow obstruction due to clamping are problematic. During clamping under forces of 20 kgf and 30 kgf, the contact area was large, and the contact area ratio was 100%, which indicated the persistence of clamping forces even after release, as well as possible blood flow obstruction. Although clamping is frequently performed with a maximum force of 30 kgf in order to affix the cable under clinical settings, the results suggested that the optimal clamping force under which blood flow remained unobstructed was less than 20 kgf. Thereafter, several specific clamping forces were examined to determine the optimal clamping force. The tightening guns displayed a minimum scale of 10 kgf and a scale of 15 kg below a scale of 20 kgf. After both of the cables, with widths of 3 mm and 5 mm, were clamped under forces of 10 kgf and 15 kgf and then released, the compressed area of the periosteum was 30% to 40%, which showed that the clamping did not obstruct blood flow over the circumference of the femoral diaphysis.
The contact pressure of the cable with a width of 5 mm was higher under a clamping force of 15 kgf, whereas no significant difference was noted in the contact pressure of the cable with a width of 3 mm. High contact pressures are not the main cause of blood flow disorders, and the contact area ratio can be used an index for biological assessments of the optimal clamping force. As the contact pressure can be an index indicating the fixity of cables in terms of conserving the fixing force, 15 kgf was judged to be more appropriate than 10 kgf. This study had some limitations in that there was no examination of contact pressures of 0.1 MPa or less. Although it was assumed that contact pressures of 0.1 MPa or less did not obstruct blood flow, the pressure of 0.1 MPa is equal to 750 mmHg, which is not low when considering blood vessels. A relevant study reported that the compression of a blood vessel under 200 mmHg led to a blood flow of 500 mg per minute [18]. Blood flow decreases with increasing pressure but is not completely obstructed even under pressures of 120 mmHg or higher [19]. This is because the application of local pressure induces vascular dilatation around the site [20]. It is necessary to examine pressures below 0.1 MPa using a sensor capable of detecting lower thresholds.
Conclusion
It is important to reduce the compressed area of the periosteum to maintain blood flow when a cable remains in contact with the femoral diaphysis after release. The clamping of UHMWPE cables under forces of 20 kgf and 30 kgf resulted in a large, compressed area, which suggested that blood flow in the periosteum might be impaired. However, impaired blood flow can be avoided through the clamping of UHMWPE cables under forces of 10 kgf and 15 kgf. Considering conservation of the fixing force, the optimal clamping force is determined to be 15 kgf.
COI
This study was funded by Alfresa Pharma Corporation (Osaka, Japan). The study sponsors did not have any involvement in the study design or collection, analyzing, or interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
References
- M Lenz, SM Perren, RG Richards, T Mückley, GO Hofmann, et (2013) Biomechanical performance of different cable and wire cerclage configuration. Int Orthop 37(1): 125-130.
- M Lenz, SM Perren, RG Richards, T Mückley, GO Hofmann, et (2013) Mechanical behavior of fixation components for periprosthetic fracture surgery. Clin Biomech 28(9-10): 988-993.
- D Wähnert, M Lenz, U Schlegel, S Perren, M Windolf (2011) Cerclage Handling for Improved Fracture A biomechanical study on the twisting procedure. Acta Chir Orthop Traumatol Cech 78(3): 208-214.
- N Tomita, S Tamai, M Shimaya, Y Mii, K Ikeuchi, et (1992) A study on elongation and knot slacking of various sutures. Bio-Medical Materials and Engineering 2(2): 71-77.
- K Hattori, N Tomita, S Tamai, Y Ikeda (2000) Bioabsorbable thread for tight tying of Journal of Orthopaedic Science 5(1): 57-63.
- I Cheng, Y Kim, MC Gupta, KH Bridwell, RK Hurford, et (2005) Apical sublaminar wires versus pedicle screws--which provides better results for surgical correction of adolescent idiopathic scoliosis? Spine (Phila Pa 1976) 30(18): 2104-2112.
- S Rosenfeld, S Kenney, E Rebich (2019) Sublaminar polyester band fixation construct in the treatment of neuromuscular J Child Orthop 13(4): 393-398.
- M Takahata, M Ito, K Abumi, Y Kotani, H Sudo, et (2007) Comparison of novel ultra-high molecular weight polyethylene tape versus conventional metal wire for sublaminar segmental fixation in the treatment of adolescent idiopathic scoliosis. J Spinal Disord Tech 20(6): 449-455.
- SS Berggren, CJ Tiderius (2015) The cedell method (cerclage wire and staple) leads to less reoperations than the AO method. A retrospective comparative study of 347 lateral ankle fractures. Acta Orthop 86(3): 384-387.
- DR Dickson, SS Mehta, D Nuttall, CY Ng (2014) A systematic review of distal interphalange al joint J Hand Microsurg 6(2): 74-84.
- S Jingushi, T Kawano, H Iida, K Oe, K Ohzono, et (2013) Reattachment of the osteotomized greater trochanter in hip surgery using an ultrahigh molecular weight polyethylene fiber cable: A multi-institutional study. Open Journal of Orthopedics 3(6): 283-289.
- NB Frisch, MA Charters, J Sikora-Klak, RF Banglmaier, DJ Oravec, et (2015) Intraoperative periprosthetic femur fracture: A biomechanical analysis of cerclage fixation. J Arthroplasty 30(8): 1449-1457.
- O Karakoyun, E Sahin, MF Erol, M Karıksız, M Küçükkaya (2016) Effect of cable cerclage on regional blood circulation in rabbits: a scintigraphic J Orthop Surg (Hong Kong) 24(3): 367-369.
- T Apivatthakakul, J Phaliphot, S Leuvitoonvechkit (2013) Percutaneous cerclage wiring, does it disrupt femoral blood supply? A cadaveric Injury 44(2): 168-174.
- R Sakai, T Yada, K Uchiyama, K Yoshida, M Ujihir (2021) The contact pressure of ultra-high-molecular-weight polyethylene cables is twice as high as that of titanium cables. Journal of Arthroscopy and Joint Surgery 8(3): 276-281.
- R Bogie, L Voss, JJ Arts, A Lataster, PC Willems, et (2016) UHMWPE Sublaminar Wires in Posterior Spinal Instrumentation Stability and Biocompatibility Assessment in an Ovine Pilot Study. Clin Spine Surg 29(10): 542-549.
- K Oe, S Jingushi, H Iida, N Tomita (2013) Evaluation of the clinical performance of ultrahigh molecular weight polyethylene fiber cable using a dog osteosynthesis Biomed Mater Eng 23(5): 329-338.
- E Friedman (1970) Choroidal Blood Flow. Pressure-Flow Relationships. Arch Ophthalmol 83(1): 95-99.
- GA Holloway, CH Daly, D Kennedy, J Chimoskey (1976) Effects of external pressure loading on human skin blood flow measured by 133Xe Appl Physiol 40(4): 597-600.
- P Abraham, B Fromy, S Merzeau, A Jardel, JL Saumet (2001) Dynamics of local pressure-induced cutaneous vasodilation in the human hand. Microvasc Res 61(1): 122-129.
