 Research Article
Research ArticleAbstract
Objectives: The aim was to estimate mortality rates, time trends by sex, and its
estimated avoidable proportion of death due to cirrhosis in Lang son Province from
2005 to 2018.
Methods: We accessed a database of population-based mortality registration
conducted yearly in 226 state health centers of 11 cities/districts of the Lang Son
province to derive 2,612 death cases during 2005-2018. The variables of each case
included the patient ID, age, sex, date, the cause of death, ICD-10 code. Mortality rates
ratio and 95% confidence interval (MRR, 95%CI), age-standardized mortality rates
(ASR), and an avoidable proportion of death were estimated.
Results: There was 88.5% of total premature deaths occurred under the age of 70.
The estimated ASR per 100,000 was remarkably higher in men (63.2) than women (7.3).
When compared to women, the estimated avoidable proportion was 88.5% of 2,321
death cases in men. The estimated mortality rates ratios, the year 2018 versus 2005,
were significantly increased in men, MRR (95%CI): 1.367 (1.104, 1.693), p=0.004; but
significantly decreased in women, MRR (95%CI): 0.344 (0.177, 0.668), p=0.002.
Conclusion: The findings suggested that Liver Cirrhosis is a preventable disease
and primary prevention and screening for the disease at an early stage would be highly
needed to reduce premature deaths occurred in communities.
Keywords: Liver Cirrhosis; Mortality Trend; Premature Death; Viet Nam
Abbreviations: CDC: Center for Diseases Control; CHS: Commune Health Stations ; ASR: Age-Standardized Rates
Introduction
During 1980-2017, Liver Cirrhosis was the major mortality of liver diseases worldwide [1]. The disease is chronic progressive liver fibrosis due to lifestyles and environmental factors [2]. In the initial stages, patients who suffered from liver cirrhosis are asymptomatic and the disease incidence rates are commonly underestimated [3]. Once clinical symptoms occur, the morbidity and premature death resulting from cirrhosis increase sharply [4]. Liver diseases due to chronic infection with hepatitis viruses [5-8] and high consumption of alcohol [9] have been observed to be common in Viet Nam from the last century to date. Harmful usage of alcohol, chronic infection with hepatitis viral infection, and smoking might be responsible for cirrhosis. Previous results have pointed out the major risk of cirrhosis was “Alcoholism” in many countries [10-13]. Based on these facts and figures, we have hypothesized that liver cirrhosis is a lifestyle-related health event and a possible avoidable disease. Patients suffering from liver cirrhosis need frequent medical care and their quality of life is affected [14]. Patients with liver cirrhosis have significantly increased morbidity and mortality [15]. However, few studies have been performed to address this public health problem in Viet Nam to date. This study aimed to estimate mortality rates, time trends by sex, and to estimate an avoidable proportion of death due to cirrhosis in men in Lang son Province from 2005 to 2018.
Methods
The study was performed in Lang Son province, a mountain
highland province in northern Viet Nam. The study population is
bordering Guangxi province in China and other provinces in Viet
Nam. It was a population-based mortality registration operated by
the Lang Son Center for Diseases Control (CDC) that covered all 226
communes of 11 cities/districts of the province, with a population
of 790,500 people in 2018 [16]. In Viet Nam, the national mortality
registration systems have been started from 1992 that was following
the guideline by the Ministry of Health to report the causes of death
from all health facilities nationwide. From 1992 to date, Lang Son
is one of all 63 cities/provinces of the country to actively conduct
mortality registration based on the medical records available
at 226 state commune health stations (CHS), 10 district general
hospitals, 9 district out-patient clinics, and 3 provincial general
and specialized hospitals. The head of the CHS is a person in charge
of the monthly report of all death cases that occurred at his/her
communes in a mortality registration book, named A6-mortality
book that was designed by the Ministry of Health. The variables
included name, age, sex, ethnicity, address, occupation, date, and
cause of death, place of death occurred (at a health facility, home,
other), and attended emergency care at the endpoint (Yes/no), and
the name of the reporter.
From 2005 to date, the Lang Son CDC has collected data from all
226 CHS using the data collection form in the hard copy of “Mortality
Registration” for six variables of name, age, sex, occupation, date,
and cause of death for every year. The additional guidelines to
determine the causes of deaths, including the immediate cause of
death, a contributing cause of death, and the underlying cause of
death, and its ICD-10 code, were sent with the designed form of
“Mortality Registration”. The average population number by sex has
also been collected by this form for every year from 2005 to 2018. A
yearly population structure by age groups of (0-9, 10-19, 20-29, 30-
39, 40-49, 50-59, 60-69, 70-79, 80+) by sex was estimated using the
results of the National Census conducted in 1999, 2009, and 2019.
The collected variables of each death case were inputted in Excel
for each district for each year. The ID and ICD-10 code for the cause
of death was made for each case. In this way, a database of mortality
from 2005 to 2018, missing data for 2009-2010, was made by the
Lang Son CDC. The dataset included 49,253 reported death cases
due to all causes [16,17].
We accessed to Lang Son database of mortality during 2005-
2018, missing data for 2009-2010, to derive variables of case’s ID,
age, sex, date, and cause of death, ICD-10 code. We found ICD-10
code K74 for Liver Cirrhosis and a total number of 2,612 cases
for the present study. We also derived the average number of
population by years and by communes for further estimate number
of person-year for the final analysis. We calculated the mortality
rates ratio with a 95% confidence interval (MRR, 95%CI) using
regression analysis, adjusted for age groups of 10-year intervals
(0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80+) and
sex. Age-standardized rates (ASR) per 100,000 person-years were
calculated using the world population structure as the standard.
We calculated the avoidable proportion of deaths in men by the
formulation of ((a-b)*100/a (a: ASR in men; b: ASR in women). The
Board of Ethics in Bio-Medical Research at University of Medicine
and Pharmacy at Ho Chi Minh City #106/UMP-BOARD, on 20 March
2019 and Hanoi Medical University Review Board in Bio-Medical
Research # 61/HMURB, on 25 November 2008 have approved the
present research protocol.
Results
Overall, a total of 2,612 deaths were registered among residents in Lang Son Province from 2005 to 2018. Table 1 shows the results of deaths were 2,321 in men and 291 in women. Men had a higher age-adjusted mortality rate (ASR-WHO 63.2 per 100,000) due to cirrhosis compared to women (ASR-WHO 7.3 per 100,000), giving man to women ratio: 8.7/1 (63.2/7.3). The estimated men to women ratio were sharply increased from 4.9/1 (49.1/10.1) in 2005 to 18.6/1 (63.1/3.5) in 2018. Compared to women, the estimated avoidable proportion of death from Liver Cirrhosis in men was ((63.2-7.3)*100)/63.2=88.5%. There was 88.5% of total premature deaths occurred under the age of 70, Table 1. The agestandardized death rate increased gradually according to WHOASR from 27.7 per 100,000 to 33.4 per 100,000 person-years for both genders from 2005 to 2018, respectively. The estimated proportion of deaths due to Liver Cirrhosis was 5.3% (2,612 cases of Liver Cirrhosis vs. 49,253 total death cases) in both genders. Overall death due to the disease, men, and women combined, was significantly increased from 2005 to 2018. After adjusting for age and sex, per-year increment was significantly seen, MRR (95%CI): 1.019 (1.009, 1.028), p=0.001 (Table 2).

Table 1: Mortality due to Liver Cirrhosis by sex during 2005-2018 in Lang Son province.
Note: Missing data for the year 2009-2010; &: Crude rate per 100,000 person-years; $: Age-standardized rate per 100,000 person-years using the World Health Organization standard population for 2000-2025; # Proportion of death cases aged under 70 year-olds. @: Age-standardized rate per 100,000 person-years using the SEGI World standard population (in the 1960s). Men to women ratio (ASRWHO) = 8.7 (63.2/7.3). The estimated proportion of death from Liver Cirrhosis in men was {(63.2-7.3)*100}/63.2=88.5%
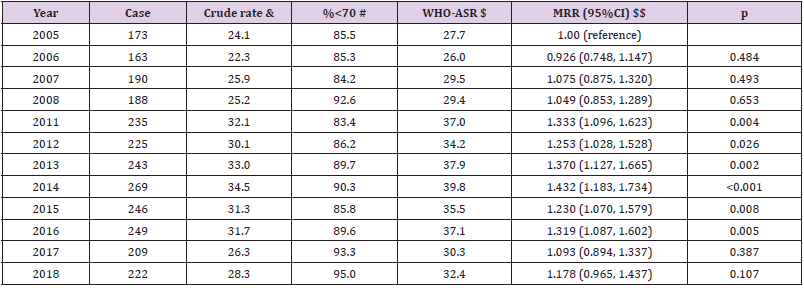
Table 2: Mortality due to Liver Cirrhosis in both genders by year from 2005 to 2018 in Lang Son province.
Note: Missing data for the year 2009-2010; the estimated proportion of deaths due to Liver Cirrhosis was 5.30% (2,612 cases of Liver Cirrhosis vs. 49,253 total cases), both genders. $$ adjusted for age group (0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80+) and sex. Per-year increment MRR (95%CI): 1.019 (1.009, 1.028), p<0.001. & Crude rate per 100,000 person-years; $ Age-standardized rate per 100,000 person-years using the World Health Organization standard population for 2000-2025; # Proportion of death cases aged under 70 year-olds. When combined all cases from 2005-2018, both genders, WHO-ASR: 31.3 per 100,000 person-years.
In men, the estimated proportion of deaths due to Liver Cirrhosis was 7.4% (2,321 cases of Liver Cirrhosis vs. 31,262 total cases). The age-standardized mortality rates per 100,000 were increased from 49.1 in 2005 to 65.1 in 2018. The estimated mortality rates ratios, the year 2018 versus 2005, were significantly increased, MRR (95%CI): 1.367 (1.104, 1.693), p=0.004. During this period, per-year increment was significantly observed, MRR (95%CI): 1.028 (1.018, 1.038), p=0.001 (Table 3). In Women, the estimated proportion of deaths due to Liver Cirrhosis was lower (1.6%, 291 cases of Liver Cirrhosis vs. 17,990 total death cases) than in men (7.4%, 2,321 cases of Liver Cirrhosis vs. 31,262 total death cases). For a time trend, in contrast, death due to the disease was significantly decreased in women from 2005 to 2018. The estimated mortality rates ratios, the year 2018 versus 2005, were significantly decreased, MRR (95%CI): 0.344 (0.177, 0.668), p=0.002. During this period, per-year decrement was significantly seen, MRR (95%CI): 0.948 (0.923, 0.974), p=0.001 (Table 4). By age-specific, the estimated mortality rates per 100,000 in men were much higher than in women for all age groups, especially for the age group (50-59), 193.5 versus 13.2, respectively (Figure 1).
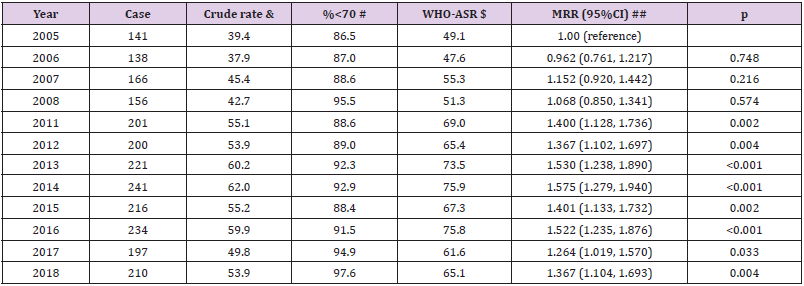
Table 3: Mortality due to Liver Cirrhosis in men by year from 2005 to 2018 in Lang Son province.
Note: Missing data for the year 2009-2010; the estimated proportion of deaths due to Liver Cirrhosis was 7.42% (2,321cases of Liver Cirrhosis vs. 31,262 total cases) in men. ## adjusted for age group (0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80+). Per-year increment MRR (95%CI): 1.028 (1.018, 1.038), p<0.001. & Crude rate per 100,000 person-years; $ Age-standardized rate per 100,000 person-years using the World Health Organization standard population for 2000-2025; # Proportion of death cases aged under 70 year-olds. When combined all cases from 2005-2018 in men, WHO-ASR: 63.2 per 100,000 person-years.
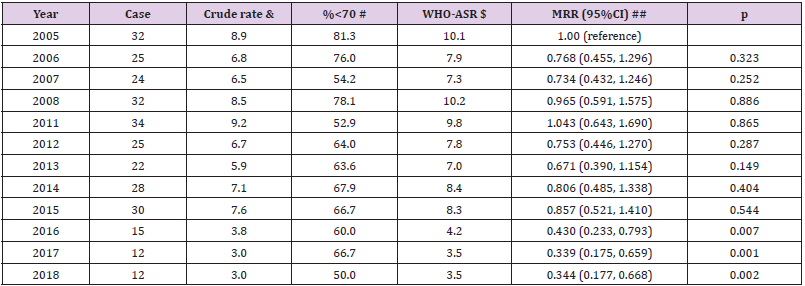
Table 4: Mortality due to Liver Cirrhosis in women by year from 2005 to 2018 in Lang Son province.
Note: Missing data for the year 2009-2010; the estimated proportion of deaths due to Liver Cirrhosis was 1.62% (291 cases of Liver Cirrhosis vs. 17,990 total cases) in women. ## adjusted for age group (0-9, 10-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80+). Per-year increment MRR (95%CI): 0.948 (0.923, 0.974), p<0.001. & Crude rate per 100,000 person-years; $ Age-standardized rate per 100,000 person-years using the World Health Organization standard population for 2000-2025; # Proportion of death cases aged under 70 year-olds. When combined all cases from 2005-2018 in women, WHO-ASR: 7.3 per 100,000 person-years.
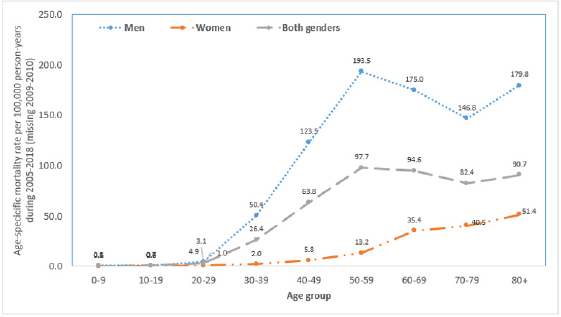
Figure 1: Age-specific mortality rate per 100,000 person-years by sex during 2005-2018 due to Liver Cirrhosis.
Note: Missing data for the year 2009-2010;
Discussion
We observed a divergence over time from 2005 to 2018 between
men (statistically significant increase) and women (statistically
significant decrease) in a community in the mountainous province
of Lang Son in northern Viet Nam. When compared to women, the
estimated avoidable proportion of death due to the disease was
about 88.5% in men. There was serious premature death, as high
as 88.5% for both genders (91.3% in men and 66.3% in women).
The findings suggested that Liver Cirrhosis is a preventable disease
and performing primary prevention in the community to reduce
premature death would be highly needed. Harmful usage of alcohol
by men living in the Lang Son province might be the major risk
factor of developing Liver Cirrhosis. An estimated annual amount
of pure alcohol consumption in 2010 was 12.1 liters and 0.2 liters in
men and women, respectively [18]. This big gap between men and
women can be consistent with the significantly higher risk of death
from Liver Cirrhosis in men than in women. Between men and
women, there were no significant differences for both Hepatitis B
virus, HBsAg positive (Odds ratio and 95% confidence interval, men
versus women: 0.76 (0.54–1.01)) and Hepatitis C virus infection
(Odds ratio and 95% confidence interval, men versus women: 1.73
0.41–7.28) [5,19].
Therefore, viral Hepatitis infection could not be explained
for the big gap between genders in the risk of death from this
disease. The present findings support our hypothesis that liver
cirrhosis is a lifestyle-related health event and a possible avoidable
disease. The results warrant further observational studies to
conclude the association between alcoholism and Liver Cirrhosis
in the disadvantaged areas in Viet Nam with emphasis on primary
prevention of the disease. There was rarely alcohol drinking (0.2%)
and tobacco smoking in Vietnamese women aged 15+ (1.7%) in
2010 [18] and it was a similar observation in the 1990s [20]. The
estimated prevalence of Hepatitis C virus infection was very low
(0.5%) in rural areas [19]. There was also a very low prevalence
(4.8%) of overweight among Vietnamese women. Therefore,
Vietnamese women will be minimized risk of Liver Cirrhosis
caused by alcoholism, smoking, Hepatitis C virus infection, and
obesity. From 2005 to 2018, nutrition and diet, living and working
environments have been improving which might be explained why
there was a significantly decreased trend of mortality from the
disease in the study population. In contrast, a significant increasing
trend in men might be related to the increasing prevalence of
harmful usage of alcohol from 25.5% in 2004 to 35.0% in 2013 [21].
The present study has several strengths, including long time of
mortality registration from 2005 to 2018 to examine time trend of
the disease; a large number of mortality cases was reported for both
men and women; the covered study population was for the entire
Lang Son province with good healthcare systems from communes
to district and provincial health facilities; mortality registration
was actively and yearly done by professional health workers; the
average population by each of 226 communes was updated for
every year that allows us to estimate the age-standardized mortality
rates by genders and for each year [16,17]. In addition, the quality
of mortality registration in Viet Nam has been validated [22-24] to
be performed well which will be feasible, reliable, and practical to
develop annual local and national mortality databases of mortality
to identify priority public health problems and to create planning
timely actions in general and in controlling Liver Cirrhosis in
particular. Based on these favorable research conditions, we can
observe a real problem of the disease and add some new pieces of
knowledge for further elimination of this preventable health threat
in our society.
Liver Cirrhosis was a serious public health problem at the
disadvantaged highland in Viet Nam of the present study population
and that was consistent with findings in the world. There were
1.32 million deaths due to Liver Cirrhosis reported in 2017, with
440,000 deaths in women and 883,000 deaths in men. The burden
of disease has been increased from 1990 to 2017. That is, the
estimated deaths due to Liver Cirrhosis were responsible for about
2.4% of total deaths in the world in 2017 compared with 1.9% in
1990 [25]. In this study, we found that mortality due to cirrhosis
was 5.3% of total deaths during 2005-2018 in the Lang Son
province that was over doubled than the world estimation. There
has been no systematic nationwide screening for Liver Cirrhosis
in Viet Nam, especially in the mountain areas, and no nationwide
comprehensive response to the disease.
The present study has certain limitations that include i)
missing data for the year 2009-2010; ii) there is no available data
of histopathological confirmation of Liver Cirrhosis, and iii) there is
not the available data of lifestyle and environmental factors related
to the disease. Despite these limitations, the present findings
warrant further studies to identify risk factors for implementing
primary prevention and secondary prevention in the community.
Source(s) of Support
There was no support.
Conflicting Interest
There are no conflicts of interest to disclose.
Acknowledgment
We are grateful to all staff of the Lang Son’s Health facilities involved in data collection, supervision, monitoring, and data management. There were no other conflicts of interest. All authors had input into the final version of the paper
References
- (2018) GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159): 1736-1788.
- Anthony PP, Ishak KG, Nayak NC, Poulsen HE, Scheuer PJ, et al. (1978) The morphology of cirrhosis. Recommendations on definition, nomenclature, and classification by a working group sponsored by the World Health Organization. J Clin Pathol 31(5): 395-414.
- Fleming KM, Aithal GP, Card TR, West J (2010) The rate of decompensation and clinical progression of disease in people with cirrhosis: a cohort study. Aliment Pharmacol Ther 32(11-12): 1343-50.
- D'Amico G, Garcia-Tsao G, Pagliaro L (2006) Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol 44(1): 217-231.
- Nguyen VT, McLaws ML, Dore GJ (2007) Highly endemic hepatitis B infection in rural Vietnam. J Gastroenterol Hepatol 22(12): 2093-100.
- Tran HT, Ushijima H, Quang VX, Phuong N, Li TC, et al. (2003) Prevalence of hepatitis virus types B through E and genotypic distribution of HBV and HCV in Ho Chi Minh City, Vietnam. Hepatol Res 26(4): 275-280.
- Hipgrave DB, Nguyen TV, Vu MH, Hoang TL, Do TD, et al. (2003) Hepatitis B infection in rural Vietnam and the implications for a national program of infant immunization. Am J Trop Med Hyg 69(3): 288-294.
- Nakata S, Song P, Duc DD, Nguyen HQ, Murata K, et al. (1994) Hepatitis C and B virus infections in populations at low or high risk in Ho Chi Minh and Hanoi, Vietnam. J Gastroenterol Hepatol 9(4): 416-419.
- Huu Bich T, Thi Quynh Nga P, Ngoc Quang L, Minh HV, NG N, et al. (2009) Patterns of alcohol consumption in diverse rural populations in the Asian region. Glob Health Action, p. 2.
- Wiegand J, Berg T (2013) The etiology, diagnosis, and prevention of liver cirrhosis: part 1 of a series on liver cirrhosis. Dtsch Arztebl Int 110(6): 85-91.
- Goncalves PL, Zago-Gomes Mda P, Marques CC, Mendonca AT, Goncalves CS, et al. (2013)Etiology of liver cirrhosis in Brazil: chronic alcoholism and hepatitis viruses in liver cirrhosis diagnosed in the state of Espirito Santo. Clinics (Sao Paulo) 68(3): 291-295.
- Bell BP, Manos MM, Zaman A, Norah Terrault, Ann Thomas, et al. (2008) The epidemiology of the newly diagnosed chronic liver disease in gastroenterology practices in the United States: results from population-based surveillance. Am J Gastroenterol 103(11): 2727-36; quiz 37.
- Mendez-Sanchez N, Aguilar-Ramirez JR, Reyes A, Dehesa M, Juorez A, et al. (2004) Etiology of liver cirrhosis in Mexico. Ann Hepatol 3(1): 30-33.
- Ge PS, Runyon BA (2016) Treatment of Patients with Cirrhosis. N Engl J Med 375(8): 767-77.
- Scaglione S, Kliethermes S, Cao G, Shoham D, Durazo R, et al. (2015) The Epidemiology of Cirrhosis in the United States: A Population-based Study. J Clin Gastroenterol 49(8): 690-696.
- Nghia LV (2020) Status of injury mortality, population-based injury mortality registration in Lang Son province, Vietnam during 2016-2018. Center for Disease Control of Lang Son province: Lang Son Provincial Health Department.
- Nghia LV (2017) Study on work-related mortality in Lang Son province during 2011-2014 [Formal Master Thesis]. Library of Hanoi Medical University: Hanoi Medical University.
- (2014) WHO (2014) World Health Organization - Cancer Country Profiles, 2014: Viet Nam.
- Nguyen VT, McLaws ML, Dore GJ (2007) Prevalence and risk factors for hepatitis C infection in rural northern Vietnam. Hepatol Int 1(3): 387-393.
- Jenkins CN, Dai PX, Ngoc DH, Kinh HV, Hoang TT, et al. (1997)Tobacco use in Vietnam. Prevalence, predictors, and the role of the transnational tobacco corporations. JAMA 277(21): 1726-1731.
- Lincoln M (2016) Alcohol and drinking cultures in Vietnam: A review. Drug Alcohol Depend 159: 1-8.
- Hong TT, Hoa NP, Walker SM, Hill PS, Rao C (2018) Completeness and reliability of mortality data in Viet Nam: Implications for the national routine health management information system. PLoS One 13(1): e0190755.
- Thuong NV, Minh LQ, Stevenson M, Linh LT, Ngoan LT (2017) Evaluation of a Population-based Intervention to Improve the Vietnamese Mortality Reporting System. Southeast-Asian J of Sciences 5(2): 194-204.
- Stevenson M, Hung DV, Hoang TH, Mai Anh L, Nguyen Thi Hong T, et al. (2015) Evaluation of the Vietnamese A6 Mortality Reporting System: All-Cause Mortality. Asia Pac J Public Health 27(7): 733-742.
- (2020) GBD 2017 Cirrhosis Collaborators. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol 5(3): 245-266.
