 Case Report
Case ReportABSTRACT
Abbreviations: EMB: Endomyocardial Biopsies; HHV6: Human Herpes Virus 6; COVID19: Coronavirus; 3D- EAM: 3 Dimensional Electroanatomical Mapping; VTs: Ventricular Tachycardias; c-MRI: Cardiac MRI
Introduction
Myocarditis is an inflammation of the cardiac muscle caused by infiltration of immunogenic cells following different kinds of cardiac injury. It most commonly results from a viral illness; however, it can also be due to non-infectious etiologies. Given its variable clinical presentation, the diagnosis is frequently missed, making it difficult to quantify the true incidence of acute myocarditis. Infectious causes include a large number of viruses, as well as bacteria, protozoa and fungi; among these pathogens viruses are the most frequent cause of the myocardial inflammatory process. The most common forms of cardiotropic viruses found in endomyocardial biopsies (EMB) are erythroparvovirus B19 (B19V) and human herpes virus 6 (HHV6) and most recently Coronavirus (COVID19) [1-4]. We will now present two cases of 3 Dimensional electroanatomical mapping (3D-EAM) guided endomyocardial biopsy for the diagnosis and therapy of B19V myocarditis presenting with ventricular arrhythmias.
Case 1
A 54-year-old woman presented to our emergency departement
with a sustained monomorphic ventricular tachycardias
(VTs) (inferior axis, RBBB, Figure 1), which, due to evolving
haemodynamic instability, had to be cardioverted externally. She
had no other known diseases except for a MTHFR mutation without
clinical relevance and did not take any medications. On her arrival
and after the external cardioversion she had no complaints. She
had a normal blood work with no signs of an active infection and
only a slightly elevated Troponin without elevation of CK as well
as CKMB. Her ECG in sinus rhythm showed a minimal diffuse STelevation
and relatively low voltages in the praecordial leads.
The patient underwent a coronary-angiography, with no signs of
coronary disease, an echocardiography which showed a normal
left ventricular function with a slightly enlarged and dyskinetic
right ventricle and finally a cardiac MRI (c-MRI) with evidence
of preserved LV function and a RV dyskinesia as well as multiple
RV aneurysms and areas of edema as well as multisegmental
transmural late gadolinium enhancement on both ventricles, setting
a differential diagnosis between sarcoidosis and myocarditis.
The patient underwent a PET-CT which ruled out the sarcoidosis.
We performed a 3DEAM-guided EMB to target areas of edema and
fibrosis on the interventricular septum and avoid false negative
results, which showed signs of an inflammatory cardiomyopathy
with B19V with active replication and started the patient on a
therapy with interferon Beta which is a well-tolerated and safe
treatment option, leading to effective virus clearance or reduction
of the virus load in patients with chronic viral cardiomyopathy [5].
After two months of therapy, we repeated a c-MRI which showed an
almost complete resolution of the edema with persistence of late
enhancement as scarred myocardial tissue. The patient underwent
a secondary prophylactic implantation of an ICD and is stable ever
since, without having experienced any new arrhythmias.
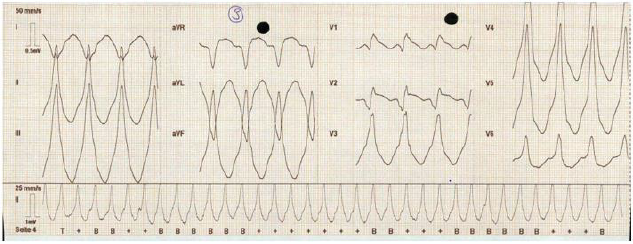
Figure 1: ECG: sustained monomorphic ventricular tachycardia with an inferior axis and a right bundle branch block, rhythm
of presentation of the patient in case1.
Case 2
A 66-year-old woman was sent to our cardiology Department
after a secondary prophylactic implantation of an ICD, due to
sustained slow ventricular arrhythmias (LSB, inferior axis) after
a probatory therapy with amiodarone as well as with sotalol. The
echocardiography showed a mildly reduced EF (41%) with a diffuse
hypocontractility, more evident in the basal segments. There were
no echocardiographic signs for a dilated cardiomyopathy or for a
hypetrophic cardiomyopathy and a coronaroangiography made
in the first hospital had already ruled out any ischaemic cause of
the reduced EF or the VTs. As the VTs were of incessant nature the
patient underwent an emergency VT ablation of the RVOT-septal
focus. Even if the procedure had an acute success with termination
of the ventricular arrhythmias, one day after the ablation the VTs
started again, and the patient was put on Mexiletine (Table 1).
Because of the unclear diagnosis of the origin of the ventricular
arrhythmias, their persistence after ablation, and the impossibility
to run a c-MRI because of the implanted ICD, we decided to perform
a 3DEAM-guided EMB which showed an active B19V replication.
We then began an immunomodulating therapy with interferonbeta,
under which a cessation of the ventricular arrhythmias was
documented. At the follow-up, after six months of interferonbeta
there were no sustained VTs anymore in the ICD-memory.
No control MRI could be performed because of the device in situ
(Figures 1 & 2).

Table 1: Endomyocardial biopsy results.
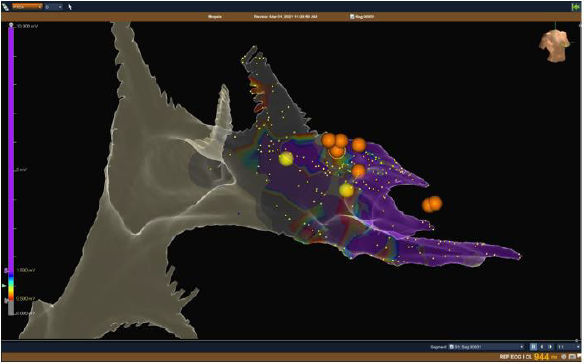
Figure 2: NavX Ensite Precision™ Image : bipolar voltage mapping of the right ventricle showing healthy ventricular tissue in
purple (bipolar voltage > 1,5 mV) and scar ventricular tissue (grey, < 0,5 mV) with pathological area identified with the color
coded scale. Right anterior oblique view with NavX Ensite Precision™ system. The yellow dots show the His Bundle
And the right fascicle
While the orange dots show the site in which the endomyocardial biopsy has been made, targetting the fibrotic or edematous
tissue on the septal right ventricular wall.
Discussion
Even though for many years the medical research has failed
to show a causative role of B19V in the genesis of heart failure
confirming only an association [5-7], some more recent works
have reported that chronic viral infections of the heart can be
one antecedent event leading to progressive dysfunction of the
myocardium, often with an impaired prognosis due to a virus- or
immune-mediated myocardial injury [6]. Moreover, even if it is
known that myocarditis can lead to cardiac dysfunction and to
ventricular arrhythmias through the development of scars and
therefore reentry circuits [8] no direct association between B19V
persistence and those clinical pictures has been described.
As the diagnosis of viral myocarditis can be problematic and
the presentation can mimic other diseases such as sarcoidosis,
arrhythmogenic cardiomyopathy as well as an evolution in dilated
cardyomyopathy, the gold standard for the diagnosis and guide of the
therapy is the EMB, an invasive but safe diagnostic tool that allows
the quantification and identification of immune cell infiltrates, the
quantification of viral loads and confirmation of virus subtypes
via sequencing [9-14]. Hystorically, the EMB was performed under
fluoroscopy guidance and was associated with potentially critical
complications such as a cardiac tamponade. In the last years,
there has been an evolving and promising use of EMB guided by
3D-electroanatomic voltage mapping, which could confere a higher
specificity and sensitivity in targeting the involved tissue and in
reducing false negative results, could reduce the radiation exposure
of patients and operators in such procedures and present a higher
safety profile compared with the mono-dimensional fluoroscopy
images [15].
We described how two patients presenting with ventricular
tachycardias of unknown cause could be successfully managed after
a diagnostic 3D-EAM guided EMB after ruling out the most common
causes of ventricular tachycardia. In our patients a subacute viral
myocarditis caused by persistent erythroparvovirus, having
sustained ventricular tachycardias as clinical presentation and
demonstrating active replication of the virus, an immunomodulating
therapy with interferon Beta was able to stabilize and resolve the
ventricular arrhythmias. The 3D EAM guided EMB either combined
with cMRI or not, can help to improve specificity and sensitivity in
targeting the involved my-ocardial tissue and avoid false negative
results, without increasing risks for the patients, as already shown
in the literature [15,16].
Conclusion
To our knowledge this is the first case series described in the literature. Even if we will need a greater number of patients to confirm our observations, we hypothesize that B19V active replication could have a pivotal role in some forms of myocarditis which show an arrhythmogenic clinical presentation and that diagnosing and treating B19V in patients with a subacute myocarditis and ventricular arrhythmias could be determinant in solving the arrhythmias as well as the myocardial inflammation, although is not curative of the areas where the myocarditis has already produced a myocardial scar. We also described the emerging role of 3DEAM-guided endomyocardial biopsy in order to target the involved myocardial tissue and reduce complications as well as false negative results.
Children with Special Needs
The term “special needs” refers to children with disabilities
who are classified into categories according to the problems they
face. These are
a) Hearing problems
b) Vision problems
c) Special learning difficulties
d) Autism
e) Mental retardation
f) Motor problems
g) Behavioral disorders
h) Speech disorders
i) Personality disorders
j) Chronic diseases [1].
Children with disabilities need in addition to special
pedagogical treatment and psychological support, which can
be achieved through the counseling process, so as to meet their
personal, educational, social and professional needs [2]. There is
no doubt that the role of counselor or psychologist is absolutely necessary so that children and adolescents feel supported and safe
in the above areas. At the same time, however, prevention must be
extended to the family system. In other words, it is necessary for the
parents of children who face some problems to seek the appropriate
counseling and psychological help, so that they can realize and at
the same time understand early on the needs of their children, but
also to support and unwind themselves psychologically.
Having a Child with Special Needs
Having a child without a doubt is one of the most important
experiences of our lives. But it ends up being the most painful, when
what we had dreamed of suddenly collapses because the child,
we brought into the world does not live up to our dreams. As a
result, completely unprepared parents view the event as a disaster,
resulting in psychological shock, which determines their later life
[3]. The treatment of this event by the parents is divided into two
phases:
a) The divisive phase according to which most parents are in a
state of shock and subconsciously often have abominable
thoughts such as for example thinking that they would prefer
their child or even to die themselves. The most common
reaction in the end is for parents to try to give birth to another
child, to make their regrets more bearable and to restore their
self-confidence and morale.
b) The recovery phase of the relationship during which there
is a variety of reactions. Most of the time the parents are
too attached to the child and consciously conflict with his
disability. In this second phase, it is necessary to be properly
informed and supported by expert counselors, so that parents
can more easily accept their child’s problem, feel relieved and
therefore be able to function more effectively [4].
Defining Counseling
The term Counseling presupposes working with individuals but also with couples, during which the counselor manages to discover as well as to explore the methods that will bring him a more creative and satisfying life [5]. This type of counseling helps parents actually discover the extent of their child’s disability and assess their developmental prospects. It also enables them to be more decisive but also to implement their decisions more effectively. Also, during the sessions, the parents learn the ways that will help them to mobilize and offer their child more help. Still, through counseling they gain more courage and thus develop over time defense mechanisms of survival. The path of early counseling, that is, according to [6] offers long-term benefits to the whole family.
The Role of the Consultant
In order for a Counselor to implement a correct counseling intervention and to give accurately and without evasions a correct information, it is certain that he must possess the necessary theoretical and practical training so that he has the ability to guide correctly as well as to support them psychologically. parents of children with special needs. The counselor must possess the correct knowledge on the disorders he is called to deal with and of course on the counseling and psychology. The main roles of the Consultant are three. Primarily, they have a therapeutic role as their job is to help people cope with this difficult phase of their lives. Their second role is a preventive role as it prevents the anticipated difficulties that the family may face in the future. The third role of the counselor is educational and evolutionary because it enables people to plan how to get the most out of their experiences which will enable them to discover and accomplish everything, they are capable of achieving. He must also accept himself to be intelligent, to be dignified and above all to be possessed by humanity and compassion.
The Role of the Parent
Nowadays parents can play an active role during their children’s rehabilitation therapy. It is easily understood that parents have the ability to observe their children’s daily behaviors that do not manifest themselves during the examination or visit to a health professional. They can also be involved during their participation in psychological support and early intervention programs and most of the time manage to have amazing therapeutic results [7]. Parents who seek and receive special help are able to act therapeutically as far as their children’s behavior is concerned and by using the programs and treatment strategies, manage to successfully deal with the difficulties that their child faces during treatment and rehabilitation. Also, parents who are trained in counseling, are able to perceive inadequate behaviors, such as speech difficulties, difficulties in self-care and behavioral issues. Thanks to the knowledge they have acquired, they are able to judge which methods are appropriate and choose them, so that they can intervene and help immediately and prevent such behaviors, such as outbursts of laughter or anger and other outbursts. In addition, they know when it is necessary to support their child and how to reach the desired behavior slowly [8].
The Advisory Process
Throughout the counseling process, it is important for parents
to be informed as clearly and accurately as possible about the
report, the diagnosis, the prognosis and the ways to deal with the
problem [8]. There are many counseling theories with similarities
and differences between them and with their own counseling
procedures. The following steps are followed in the counseling
process in which the Counselor and the Counselor participate.
1) Stage 1: The Counseling process begins with the first contact
of the counselor and the Counselor, who by creating a good
psychological climate, set the desired goals.
2) 2nd Stage: In this stage, the relationship between the Consultant
and the Consultant is built, which is the most important
element that will lead to the success of the counseling process.
Here the Consultant has the dominant role, since he is the one
who with his correct behavior should facilitate the smooth
outcome of the process. This will be achieved more easily,
since it positively affects the Counselor, who, by adopting his
personal way of thinking, now helps and believes in himself.
The purpose of this second stage is to create the right climate
of trust that will help parents express how they feel, express
doubts and discuss the goals they have set for their child.
3) Stage 3: This stage leads through the development of a positive
relationship between the Consultant and the Consultants in
setting and delimiting the goals.
4) Stage 4: After setting the goals, the Consultant, taking into
account the personalities of himself and the Consultant, applies
his scientific knowledge in order to choose the appropriate
consulting method.
5) 5th Stage: This stage is the end of the whole counseling
process. This process is therefore considered successful when
the initial goals have been achieved.
Conclusion
With the right guidance and support of families of children with special needs, it is possible in our time, as we saw above, for these families to find their own tactics for solving the problems they face as well as to use various techniques in their personal daily lives. You put more emphasis on these elements of the family that are considered more positive as well as on gaining in terms of selfconfidence [2]. In other words, counseling for families with children with special needs, whether it is some kind of disability or a special learning disability, can offer a better quality of life, peace of mind and clarity in order to help the child properly and effectively.
References
- Kuhl U, Pauschinger M, Noutsias M, Seeberg B, Bock T, et al. (2005) High prevalence of viral genomes and multiple vi-ral infections in the myocardium of adults with ‘idiopathic’ left ventricular dysfunction. Circu-lation 111(7): 887-893.
- Kuhl U, Pauschinger M, Seeberg B, Lassner D, Noutsias M, et al. (2005) Viral persistence in the myocardium is associated with progressive cardiac dysfunction. Circulation 112(13): 1965-1970.
- Verdonschot J, Hazebroek M, Merken J, Debing Y, Dennert R, et al. (2016) Relevance of cardiac parvovirus B19 in my-ocarditis and dilated cardiomyopathy: review of the literature. Eur J Heart Fail 18: 1430-1441.
- Teresa Castiello, Georgiopoulos G, Finocchiaro G, Claudia M, Gianatti A, et al. (2021) COVID-19 and myocarditis: a systematic review and overview of current challenges. Heart Fail Rev 24: 1-11.
- Heinz peter Schultheisset, Piper C, Sowade O, Waagstein F, Kapp JF, et al. (2016) Betaferon in chronic viral cardiomyopathy (BICC) trial: Effects of interferon-β treatment in patients with chronic viral cardiomyopathy. Clinical research in cardiology 105(9): 763-773.
- Michael H Chiu, Cvetan Trpkov, Saman Rezazedeh, Derek S Chew (2019) Monomorphic Ventricular Tachycardia as a Presentation of Giant Cell Myocarditis. Case Rep Cardiol 2019: 7276516.
- Garrick C Stewart, Molina JL, Gottumukkala RVS RK, Rosner GF, Anello MS, et al. (2011) Myocardial Parvovirus B19 Persistence Lack of Association With Clinicopathologic Phenotype in Adults With Heart Failure. Circulation: Heart Failure 4(1): 71-78.
- Van Linthout S, Tschope C, Schultheiss HP (2014) Lack in treatment options for virus-induced inflammatory cardiomyopathy: can iPS-derived cardiomyocytes close the gap? Circ Res 115(6): 540-541.
- Holzmann M, Nicko A, Kuhl U, Noutsias M, Poller W, et al. (2008) Complication rate of right ventricular endomyocardial biopsy via the femoral approach: a retrospective and pro- spective study analyzing 3048 di-agnostic procedures over an 11-year period. Circulation 118(7): 1722-1728.
- Chimenti C, Frustaci A (2013) Contribution and risks of left ventricular endomyo- cardial biopsy in patients with cardiomyopathies: a retrospective study over a 28-year period. Circulation 128(14): 1531-1541.
- Caforio AL, Pankuweit S, Arbustini E, Basso C, Blanes JG, et al. (2013) Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: a position statement of the European Society of Cardiology Working Group on Myo- cardial and Pericardial Diseases. Eur Heart J 34(33): 2636-2648; 2648a-2648d.
- Kuhl U, Schultheiss HP (2010) Myocarditis in children. Heart Fail Clin 6: 483-496; viii – ix.
- Kuhl U, Lassner D, Dorner A, Rohde M, Escher F, et al. (2013) A distinct subgroup of cardiomyopathy patients characterized by transcriptionally active cardiotropic erythrovirus and altered cardiac gene expres-sion. Basic Res Cardiol 108(5): 372.
- Tschope C, Kherad B, Schultheiss HP (2015) How to perform an endomyocardial biopsy? Turk Kardiyol Dern Ars 43(6): 572-575.
- Michela Casella, Russo AD, Bergonti M, Catto V, Conte E, et al. (2020) Diagnostic Yield of Electroanatomic Voltage Mapping in Guiding Endomyocardial Biopsies. Circulation 142(13): 1249-1260.
- Vaidya VR, Abudan AA, Vasudevan K, Shantha G, Cooper LT, et al. (2018) The efficacy and safety of electroanatomic mapping-guided endomyocardial biopsy: a systematic review. J Interv Card Electrophysiol 53(1): 63-71.
