info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map

Received: October 28, 2017; Published: November 03, 2017
Corresponding author: Faaiz Ali Shah, MBBS,FCPS (Orthopedics), Assistant Professor, Orthopedics & Trauma, Lady reading Hospital Peshawar, KP, Pakistan
DOI: 10.26717/BJSTR.2017.01.000495
The larva of the tap worm Echinococcus Granulosus causes Hydatid Cystic disease in humans which is a common public health problem in many countries of the Middle east, Mediterranean, Australia and New Zealand [1,2]. The cyst of the tapworm can be found anywhere in the body but liver (55 to 70%) and lungs (20 to 30%) are more commonly affected by the tape worm.1 The viscera of the body like heart, kidneys, spleen and brain and are very rarely affected by the disease and even rarer are the skeletal muscles which are affected in only 1 to 4% of the cases [3]. We present a case report of hydatid disease which involved the paraspinal muscles of the lumbar back without any involvement of liver or lungs.
A 35 years old lady was referred by a general surgeon with chief complaints of pain and diffuses swelling on right side of par vertebral muscles in the lumbar area. She was a febrile and the swelling was not associated with any trauma. Her general health status was satisfactory. Examination reveals a diffuse and non-tender swelling in the right side of paraspinal muscles in the lumbar area. It was adherent to muscles. It was cystic in consistency. Neurological examination was normal. On blood complete examination was normal. Chest radiographs and abdominal ultrasound was normal. The diagnosis of hydatid cyst was strongly suspected on ultrasound examination, which showed multiloculated cystic mass in the para vertebral muscles in lumbar area. MRI of lumbar spine showed a multilocularis cystic lesion in the para spinal muscles on right side of lumbar area (Figures 1 & 2).The intact intramuscular cyst was completely excised. The cavity was thoroughly irrigated with hypertonic saline. A histopathological examination confirmed hydatid cyst. Postoperatively, the patient began receiving albendazol 400 mg twice daily, for 6 months and no recurrence reported (Figures 3 & 4).
Figure 1: Sagittal MRI Lumbar area showing Multiloculated Hydatoid Cyst.
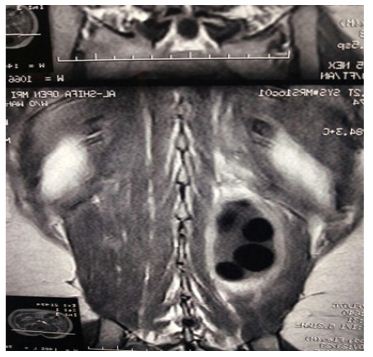
Figure 2: Coronol MRI showing Hydatoid Cyst.
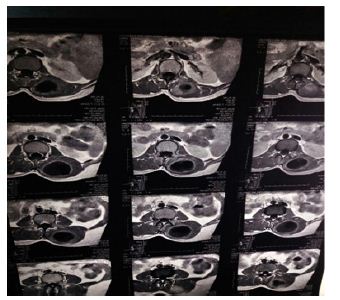
Figure 3: Hydatoid Cyst after removal through surgery.

Figure 4: Hydatoid cyst after removal (approximate size).

Hydatid cystic disease commonly known as Hydatidosis or Echinococcosis is frequently found in sheep-raising countries like Australia, Greece, South America, China and India but cases are reported in developed countries as well [4,5]. Humans are most commonly affected by the larva of tapeworm Echinococcus Granulosus followed by Echinococcus Multilocularis, and Echinococcus Vogeli [6,7]. The pathogenesis of Hydatid cyst in muscles is not clearly known. Various theories have been proposed. Some researchers believe that direct contact of the larva with the wound as in dog bite can be the possible explanation, while others proposed that larva is transferred to the muscles via blood stream from primary source in liver and lungs.(10 to 15% cases) [8]. Still others are of the opinion that larva is transported across the muscular layer of gut into the venous system bypassing liver [9,10]. Clinical features of Hydatoid cyst varies from the presence of a swelling or mass to pressure symptoms, cyst infection and rarely anaphylactic shock [1]. In our patient there was no pressure symptom except a growing mass in lower back muscles which suggests a higher suspicion of Hydatid cyst in any growing mass in muscles. The investigation of choice for diagnosing Hydatid cyst is MRI which shows a thin walled cyst with no septation and containing numerous daughter cysts inside [11] Some radiological features distinguish Hydatid cyst from other cysts and these include the “Rim sign” [12] which is a low intensity signal around the cyst,” the Bunch of Grapes” sign [13] which is the hypo intense wall of the cyst on T1 and T2 images without septation and enhancement and the “Water lily sign” which denotes the detached germinal layer of the cyst wall [9].
Biochemical blood tests uses complement fixation and ELISA helps in diagnosis [14-15]. In our case the Casoni serological test was positive. Muscular Hydatid cysts are surgically removed with a wide clear margin [16]. Failure to achieve radical excision of the muscular cyst results in non-healing of wound and may require re surgery [12]. Administration of benzimidazole pre and post operatively is recommended. We were able to excise the cyst radically in our patient without any complication. Because of the difficulty of radical resection of muscular cysts and increase morbidity associated with this procedure, Biljic [17] percutaneous drain a cyst in Para spinal muscles followed by 95% ethanol injection and reported no recurrence or any complication in his 26 months follow up with this PAIR(puncture, aspiration, injection, re-aspiration) technique. However his technique is not being used in large number of patients and needs expertise as well. It is suggested that in order to prevent recurrence and complications the cyst should be removed intact but which is not always possible therefore local irrigation with formalin, aqueous iodine, silver nitrate and hypertonic solution is advocated in accidental rupture of cyst or spillage of cyst contents [13]. We recommend that hydatid cyst disease should be considered in the differential diagnosis of any lumbar muscular swelling and to confirm the diagnosis complete history, examination, serological tests and radiological investigations are necessary followed by surgical excision with wide margins to prevent recurrence.


























