info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map

Received: August 23, 2017; Published: September 08, 2017
Corresponding author: Jayesh V Trivedi, Head of department and professor of medicine, Gujarat adani institute of medical science, Bhuj, Gujarat, India
DOI: 10.26717/BJSTR.2017.01.000339
Aortic dissection occurs in 3 in 100,000 people per year. Tear in the inner side of aorta causes blood to flow between layers of aorta causing seperation of media layer into inner two third and outer one third. Dissection can be antegrade or retrograde.
96% of people will have chest pain with varying severity with or without radiation. Back pain, vomiting, sweating, headache, blood stained diarrhea, paralytic ileus, strokes and death Males are more affected than females. Males will have double incidence as females.
Hypertensions in 80% of patients were observed. A connective tissue disorder is also common. Bicuspid Aortic valve is seen in 7to14% of patients. 5To9% of patients has Marfan syndrome. Along with this Atherosclerosis, Trauma, Post cardiac surgery, Smoking, Cocaine abusers, pregnancy, Aortoarteritis, Turners syndrome, High intensity weightlifting, Syphilis are the other causes [1-7].
D dimer more than 500 ng/ml rules out Aortic dissection. Transoesophageal echocardiogram helps in diagnosing the sensitivity is 98% and specificity is 97%. Ultrasound of abdomen, computerized Tomography, Magnetic resonant Angiography will diagnose Aortic dissection, the sensitivity is 98% and specificity is 98%. This is being classified in to Stanford Type A. Where ascending and arch of aortas are affected. Stanford Type B...where ascending aorta is spared.
It is also classified in De Bakey classification as
A. Type 1. Dissection originates in ascending aorta. It occurs in patients less than 65 yrs of age.
B. Type 2. Dissction originates in ascending aorta and extends distally.
C. Type 3.Dissection occurs in descending aorta and rarely extends. This is commonly seen in patient having Hypertension and Atherosclerosis.
Control Hypertension by either Betablockers, sodium nitroprusside, Calcium channel blockers like Diltiazem or verapamil, nonpyridine calcium channel blockers. Target mean arterial blood pressure should be 60 to75 mm of hg. Initial decrease should be about 20%. Patient emotional care and reduction in psychological stress is equally important along with medical treatment. Surgical treatment either Endovascular or open surgery may be necessary in acute emergencies (Figures 1-5).
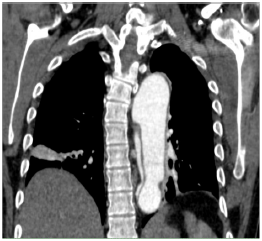
Figure 1: Severe hypotension in acute dissection indicates grave prognosis.

Figure 2: Aortic Dissection in Descending Aorta.
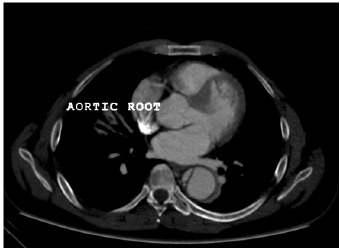
Figure 3: Aortic Dissection In Descending Aorta.
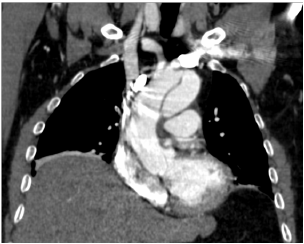
Figure 4: Dissction Ao Root.
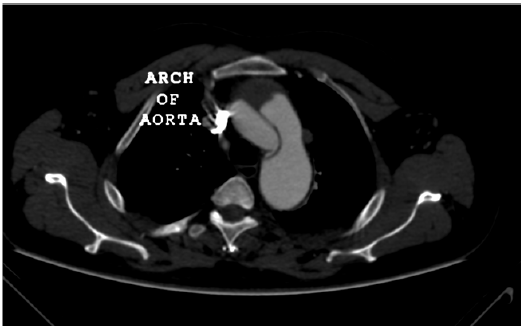
Figure 5: Dissection in Ascending Aorta And Arch Of Aorta.
Tight Bp controls, avoid smoking, maintain ideal weight, wear a suit belt, regular medical checkup and control of dyslipidemia are important. Severe hypotension in acute dissection indicates grave prognosis.


























