info@biomedres.us
+1 (502) 904-2126
One Westbrook Corporate Center, Suite 300, Westchester, IL 60154, USA
Site Map

Received: August 03, 2017; Published: August 09, 2017
Corresponding author: Hakan Bilhan, Associate Professor at the Okan University Faculty of Dentistry, Department of Prosthodontics, Gulbahar Mh, Oya Sok No: 23/A, Mecidiyekoy, Sisli, Istanbul 34394, Turkey
DOI: 10.26717/BJSTR.2017.01.000262
Immediate Loading is mostly appreciated by patients, since they do not have to stay edentulous until the osseointegration. For this purpose there must be an implant system providing abutments suitable for screw retention and a prefabricated restoration. In this case report the procedures for this treatment modality are described in a detailed way. Additionally, the return from fixed to removable upon request of the patient due to easier cleaning was explained, too. The lab procedures and the makeover to a telescopic denture was looked into in this case report.
A 70 year old male patient with mandibular teeth showing a poor prognosis due to chronic generalised periodontitis was chosen to treat with a fixed detachable prosthesis [1] supported with 4 implants after extraction of all remaining teeth. Since the lower jaw was causing the main problem, the maxillary treatment was postponed for later on.
Figure 1: Matching and Planning.
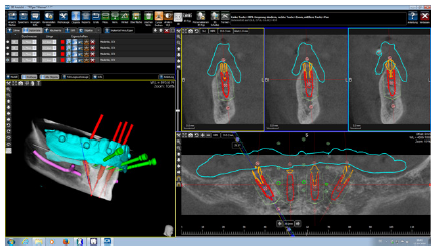
A preoperative 3-D planning was performed with the help of Dental Volumetric Tomographies (DVT, Galileos Comfort Plus, Dentsply Sirona, Bensheim, Germany) and with the planning software for Guided Surgery (Magellan, Medentis Medical, Bad Neuenahr – Ahrweiler, Germany) (Figure 1).
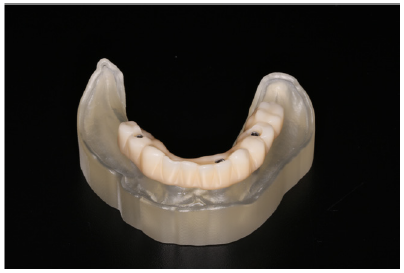
Based on the planning a printed model (Figure 2), surgical guides and a CAD/CAM milled PMMA provisional (Figure 3) were fabricated.
Figure 2: 3D printed model.

Figure 3: PMMA Provisional, view from facial.
The surgical part was achieved with surgical guides making the placement of dental implants flapless and exactly in the same position as originally planned [2,3]. Implantation in the positions 34, 32, 42, 44 with immediate loading via a milled prefabricated PMMA provisional which is a high performance acrylic (ICX- Smile Bridge, Medentis Medical, Bad Neuenahr – Ahrweiler, Germany) was accomplished. This technique is not new; it was introduced by Malo and colleagues [4]. Following this protocol, the implants in the positions 32 and 42 were placed straight, whereas the distal implants were placed with an angle of 35 degrees (positions 34 and 44). The use of angulated implants gives the possibility to prevent complicated sinus lifting or augmentation procedures and protect anatomic structures such as the foramen mentale. The used implant system gives the possibility to use two different degrees: 17 or 35.
It is important to achieve a primary stability of the implants of at least 35 Ncm, to be able to load them immediately [5-7].
The next step was to mount the occlusally screwed abutments (Multi Abutment, Medentis Medical, Bad Neuenahr – Ahrweiler, Germany) on the implants and take care of the right gingival height. After checking the fit and occlusal stability of the Smile-Bridge, the fixation intraorally was succeeded with an autopolymerising denture repair polymer of diacrylate base (QU-resin,Bredent, Senden, Germany). After torque-wrenching of the fixation screws, the screw holes were closed with a light-cured provisional material (TELIO CS Inlay, Ivoclar Vivadent,Schaan,Liechtenstein).
3 months later, it was time for the definitive prosthetic treatment. Although a detachable prosthesis was planned originally, the treatment direction was changed, since the patient was complaining of food trapping and difficulties in cleaning underneath.
Since the used system was providing the possibility of fabricating and working on occlusally screwed abutments for Ti Base supported telescopic prosthesis, it was possible to workon workon on abutment level. On the model with the abutment level implant analogues, Ti-Bases were used for the fabrication of conical abutments with 20 of divergence angle. The margins of the telescopic crowns were established 1mm supragingivally. The height of the primary crown structures were arranged at 6mm’s and the insertion pathway was determined (Figure 4). The milled (CAD/CAM-System: inLab SW 15.0, Dentsply Sirona, Bensheim, Germany) zirconia (IPS E.max ZirCAD, Ivoclar Vivadent, Schaan, Liechtenstein) structure (Figure 5a) was bonded to the titanium basis (Hera Attachment Bond, Heraeus Kulzer GmbH, Hanau, Germany). The removable structure was fabricated upon these abutments carrying the Galvano produced secondary parts. The galvano secondaries (Figure 5b) were cemented in the removable part intraorally (Figure 6a-6c) in order to prevent any tension and to achieve a passive fit [8]. The CrCo-alloy substructure (Figure 7) was cast from a 3-D printed premodel (Figure 8).
Figure 4: Computer Aided Design.
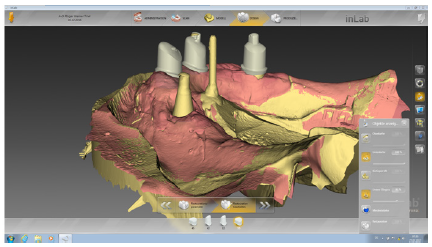
Figure 5a: Zirkonia abutments.
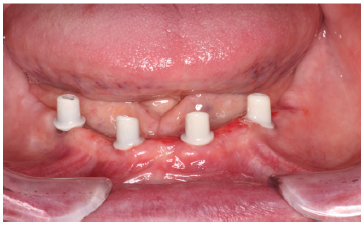
Figure 5b: Galvanos in situ.
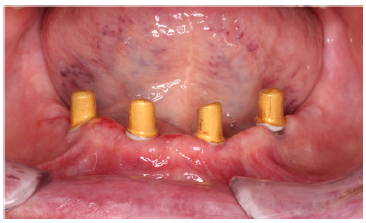
Figure 6a:Mixing the dualcure cement.
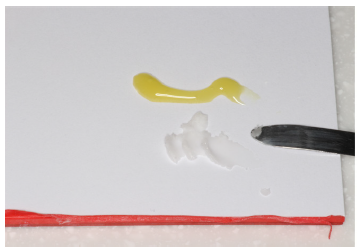
Figure 6b:Zirkonia abutments.

Figure 6c:Fixation of the tertiary structure intraorally.

Figure 7:Superstructure made of nonprecious alloy during try-in.
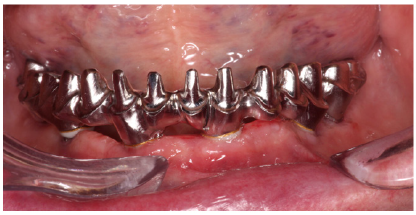
Figure 8:3-D printed pre-model.

The different approach during the whole removable prosthesis part, was the use of single Emax crowns (IPS E.max CAD, Ivoclar Vivadent, Schaan, Liechtenstein) instead of prefabricated porcelain denture teeth (Figure 9). It was a more economic solution in this case, since the clinic owned a lab with its own CAD/CAM and milling unit. The Emax crowns offered great esthetics and toughness, as well as ease of repair, since the related data were recorded and kept for remaking any time.
Figure 9:Final Restoration.

Immediate Loading with a fixed solution is a well appreciated treatment for patients, since the osseointegration time is overlapped with teeth mimicking real life and esthetic and functional demands are successfully fulfilled. Today preimplantolgical diagnostic and planning possibilities enable clinicians to prepare fully for the postimplantation procedures.
It should be kept in mind that, not seldom, patients can be unhappy or disappointed with their fixed detachable dentures due to missing buccal flanges causing an unsupported lip, phonation problems depending on a fully open palate or difficult cleaning procedures with the fixed solution.
In this manner, clinicians should be flexible in switching to the removable denture option. For this purpose, it is advisable to use a system which allows working on occlusally screwed abutment level, so that the same abutments may be used for the locators or telescopic solutions.
Another innovative step in this case was to use lithium disilicate crowns instead of prefabricated porcelain crowns. This was for a dental clinic owning a milling unit and an own lab, a more economic and safe way to go. The saved data can be used any time to replace a chipped or fractured porcelain tooth. Telescopic dentures are a well documented treatment alternative among removable dentures. The use of Ti-Base supported zirconia conus abutment is a cost effective solution.
It seems to be an important issue to investigate what percent of the edentulous patients is satisfied with the delivered fixed restoration and how many of them prefer to return to the removable denture status.


























